| Journal of Neurology Research, ISSN 1923-2845 print, 1923-2853 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Neurol Res and Elmer Press Inc |
| Journal website https://jnr.elmerpub.com |
Review
Volume 16, Number 1, March 2026, pages 9-21

Traumatic Brain Injury and Its Impact on Personality and Behavior: A Narrative Review
Muhammad Saeeda ![]() , Sumaiyya Syedab
, Sumaiyya Syedab ![]() , Muhammad Umar Ahsana
, Muhammad Umar Ahsana ![]() , Maha Ahmedc
, Maha Ahmedc ![]() , Manognya Gaddamd
, Manognya Gaddamd ![]() , Lea Nohrae
, Lea Nohrae ![]() , Sourav Paulf, k
, Sourav Paulf, k ![]() , Kanchan Chaudharyg
, Kanchan Chaudharyg ![]() , Muniba Syedh
, Muniba Syedh ![]() , Sara Ajamii
, Sara Ajamii ![]() , Rabbea Alij
, Rabbea Alij ![]() , Aghna Imanc
, Aghna Imanc ![]()
aD. G. Khan Medical College, Dera Ghazi Khan, Pakistan
bFaculty of Medicine, Georgian National University (SEU), Georgia
cShaheed Mohtarma Benazir Bhutto Medical College Lyari, Karachi, Pakistan
dMamata Academy of Medical Sciences, Hyderabad, India
eFaculty of Medical Sciences, Lebanese University, Beirut, Lebanon
fFaridpur Medical College, Faridpur, Bangladesh
gLiaqat University of Medical and Health Sciences, Jamshoro, Pakistan
hCMH Lahore Medical College, Lahore, Pakistan
iAmerican University of Beirut, Beirut, Lebanon
jKing Edward Medical University, Gumbad Lahore, Pakistan
kCorresponding Author: Sourav Paul, Faridpur Medical College, Faridpur, Bangladesh
Manuscript submitted November 3, 2025, accepted February 9, 2026, published online March 13, 2026
Short title: TBI and Its Impact on Personality and Behavior
doi: https://doi.org/10.14740/jnr1058
| Abstract | ▴Top |
Traumatic brain injury (TBI) is a leading cause of long-term disability worldwide, contributing to significant neurological, psychological, and social impairments. Beyond the physical and cognitive consequences, TBI profoundly affects personality and behavior, influencing emotional regulation, social functioning, and overall quality of life. This narrative review synthesizes current evidence on the epidemiology, pathophysiology, and neuropsychiatric consequences of TBI, with a particular focus on the mechanisms and clinical implications of personality and behavioral changes following injury. A comprehensive literature search was conducted using PubMed, Cochrane Library, and Scopus databases up to December 31, 2024. Relevant studies, including randomized controlled trials, cohort studies, and reviews, were analyzed to summarize key findings related to TBI-induced neurobiological mechanisms, behavioral outcomes, and rehabilitation approaches. TBI severity and lesion localization, especially within the frontal and temporal lobes, were found to critically determine the nature of post-injury personality alterations, including impulsivity, aggression, apathy, and emotional dysregulation. These manifestations are mediated by disruptions in dopaminergic and GABAergic neurotransmission and by secondary injury mechanisms such as oxidative stress, excitotoxicity, and neuroinflammation. Behavioral sequelae frequently co-occur with psychiatric disorders such as depression, anxiety, and substance use, complicating recovery. Rehabilitation outcomes are optimized through interdisciplinary interventions integrating cognitive-behavioral therapy, pharmacologic modulation, and family-centered care. Personality and behavioral changes after TBI represent a major determinant of social reintegration and quality of life. A deeper understanding of the neurobiological underpinnings and psychosocial moderators is essential for personalizing rehabilitation strategies. Future research should emphasize longitudinal, multicenter studies and ethical frameworks that support comprehensive, person-centered neurorehabilitation.
Keywords: Traumatic brain injury; Personality changes; Behavioral changes; Neurobiological mechanism
| Introduction | ▴Top |
Traumatic brain injury (TBI) is a serious public health issue that occurs when an external force acts on the brain and inhibits its normal function [1]. TBI can range from mild concussion to severe TBI and coma or death, depending on the injury site and extent of damage to the brain. Common causes of TBI include falls, motor vehicle accidents, assaults, and sport-related injuries, although military personnel are still vulnerable to TBI from explosive blasts [2]. Diagnosis is based on clinical evaluation and imaging techniques (e.g., computed tomography (CT) for acute screening, magnetic resonance imaging (MRI) for detecting subtle lesions). TBI will also result in both acute and chronic sensorimotor, psychological, and cognitive deficits [3]. Recently, epidemiological evidence has indicated that TBI is a significant risk factor for neurodegenerative diseases. Meta-analyses have estimated an approximately 70% increased risk of dementia after TBI [4], and some more recent reviews suggest that the risk may be as high as four times in certain populations [5].
TBI severity is conventionally classified with several parameters. The Glasgow Coma Scale (GCS) is the standard measure, with mild TBI defined as GCS score of 14–15, moderate TBI as GCS 9–13, and severe TBI as GCS 3–8 [6]. Of course, GCS may not always be available or accurate, which can introduce an element of confusion when evaluating a person who is sedated or intoxicated. To fill this gap, the Mayo Classification System includes other parameters, such as neuroimaging abnormalities, time of loss of consciousness, and post-concussion symptoms, in formulating a more complete approach for severity assessment [7]. Additionally, newly defined mild TBI measure altered mental status, amnesia, and neurologic deficits that would support parallel diagnosis and comparisons of research [8]. These classifications are essential to clinical practice and, more importantly, address research design.
TBI represents a significant burden worldwide, and its epidemiology differs by age, sex and region. According to the Global Burden of Disease (GBD) 2021, there were an estimated 20.8 million new cases of TBI around the world, with an age-standardized incidence of 259 per 100,000. Males consistently have higher incidence rates, and falls are the leading cause worldwide, particularly in older populations. Regionally, Eastern Europe and some regions in the Middle East appear to have the highest burden [9]. In 2019, GBD estimated that there were 27.2 million incident cases and 48.9 million prevalent cases of TBI and 7.1 million years lived with disability (YLDs) attributable to TBI worldwide [10]. Not only do these figures demonstrate acute harmful effects of TBI on individuals, but collectively TBI has chronic impacts on individuals and health systems.
TBI can result in clinical sequelae beyond physical injury. It can profoundly change how survivors behave, think socially, and function personally and emotionally [11]. These changes may lead to significant disability and, in some cases, may persist longer than physical injury itself. Some of these changes are related to organic brain damage, whereas others depend on patient’s emotional and psychological adaptation to their disabilities [12]. These changes can be better understood if viewed through a neuroanatomical framework, which helps educate patients and families by associating identity and selfhood to neurophysiology, as opposed to a more abstract philosophical construct [13]. Typical cognitive deficits associated with TBI include a slowing process of information, memory deficits, attention deficits, and executive dysfunction [14]. Rehabilitation is multidisciplinary in scope, encompassing daily living retraining, cognitive and behavioral intervention, and family systems approaches.
Even mild TBI can produce persistent symptoms described as post-concussion syndrome. There is still a gap in knowledge regarding TBI, especially related to pathophysiological differences between children and adults with TBI. The developing brain has different pathways for injury, such as increased vulnerability to axonal injury and excitotoxicity that is more diffuse in nature, which speaks to the need for dedicated pediatric research and pediatric clinical trials [15]. There is also an increased incidence of, and poor outcomes from TBI among Indigenous populations, with culturally specific rehabilitative methods yet to be researched, which further diminishes equitable outreach for care. In low- and middle-income countries (LMICs), TBI carries a high burden and poor outcomes, largely due to limited structures to prevent TBI [16].
Overall treatment paradigms for TBI remain incomplete, as a standard of effective pharmacologic neuroprotective treatments remain unfulfilled despite great investment in TBI research. The aim of this narrative review was to provide a synthesis of existing knowledge of TBI’s epidemiology, classification of TBI, and the complex relationship with personality and behavioral pathology. This review stresses the need for personalized treatments that utilize both psychological intervention and medical therapy. To effectively personalize treatment of TBI, we argue that a comprehensive neuropsychological assessment is needed in order to assess the remaining and impaired capabilities, which is paramount for prognostics, treatment planning, and improving long-term patient outcomes [17].
| Methodology | ▴Top |
We conducted a narrative literature review using PubMed, Cochrane Library, and Scopus databases from inception to December 31, 2024, with the following keywords: “traumatic brain injury,” “mild traumatic brain injury,” “diffuse axonal injury,” “neurocognitive outcomes after TBI,” “psychiatric sequelae of TBI,” “rehabilitation after TBI,” and “global burden of TBI.” The literature search included cross-sectional studies, randomized controlled trials, cohort studies, case reports, and review articles published in English. Emphasis was placed on publications from the last decade; however, earlier articles of significant scientific or clinical relevance were not excluded.
To ensure comprehensive coverage, we manually reviewed the reference lists of all included studies, reviews, and relevant book chapters to identify additional eligible publications. The inclusion criteria were studies involving participants aged 18 years and above with diagnosed TBI. Studies exclusively addressing pediatric populations or unrelated neurological conditions were excluded unless they specifically addressed mechanisms or outcomes relevant to TBI.
This narrative review sought to synthesize current evidence regarding epidemiology, pathophysiology, clinical outcomes, neuropsychiatric consequences, and management strategies associated with TBI.
| Mechanism of TBI | ▴Top |
Primary injury
Primary injury occurs during a traumatic event and is caused by direct mechanical forces, such as blow, acceleration/deceleration, penetration.
Focal brain injury
It is caused by collision forces applied to the skull and subsequently compressing the tissue below the cranial vault from the impact location (coup) or of the tissue opposite of the site of impact (contrecoup) [18].
Diffuse brain injury
It is caused mainly by rapid acceleration–deceleration or rotational forces, leading to widespread brain involvement such as diffuse axonal injury (DAI) and cerebral swelling [19, 20].
Secondary injury
Secondary injury occurs within minutes to days following primary trauma and consists of metabolic and cellular changes that worsen injury [21]: 1) ischemia and hypoxia (lack of blood and oxygen to the brain); 2) excitotoxicity (excess glutamate release leading to neuronal injury [22]); 3) mitochondrial dysfunction (decreased ATP generation and cell death); 4) oxidative stress (damage to cells from free radicals [23]); 5) neuroinflammation (activation of microglia and the release of cytokines [24]); 6) cerebral edema (swelling increasing intracranial pressure (ICP) which can lead to herniation); and 7) blood-brain barrier (BBB) breakdown allowing harmful substances to enter, worsening injury [25] (Fig. 1).
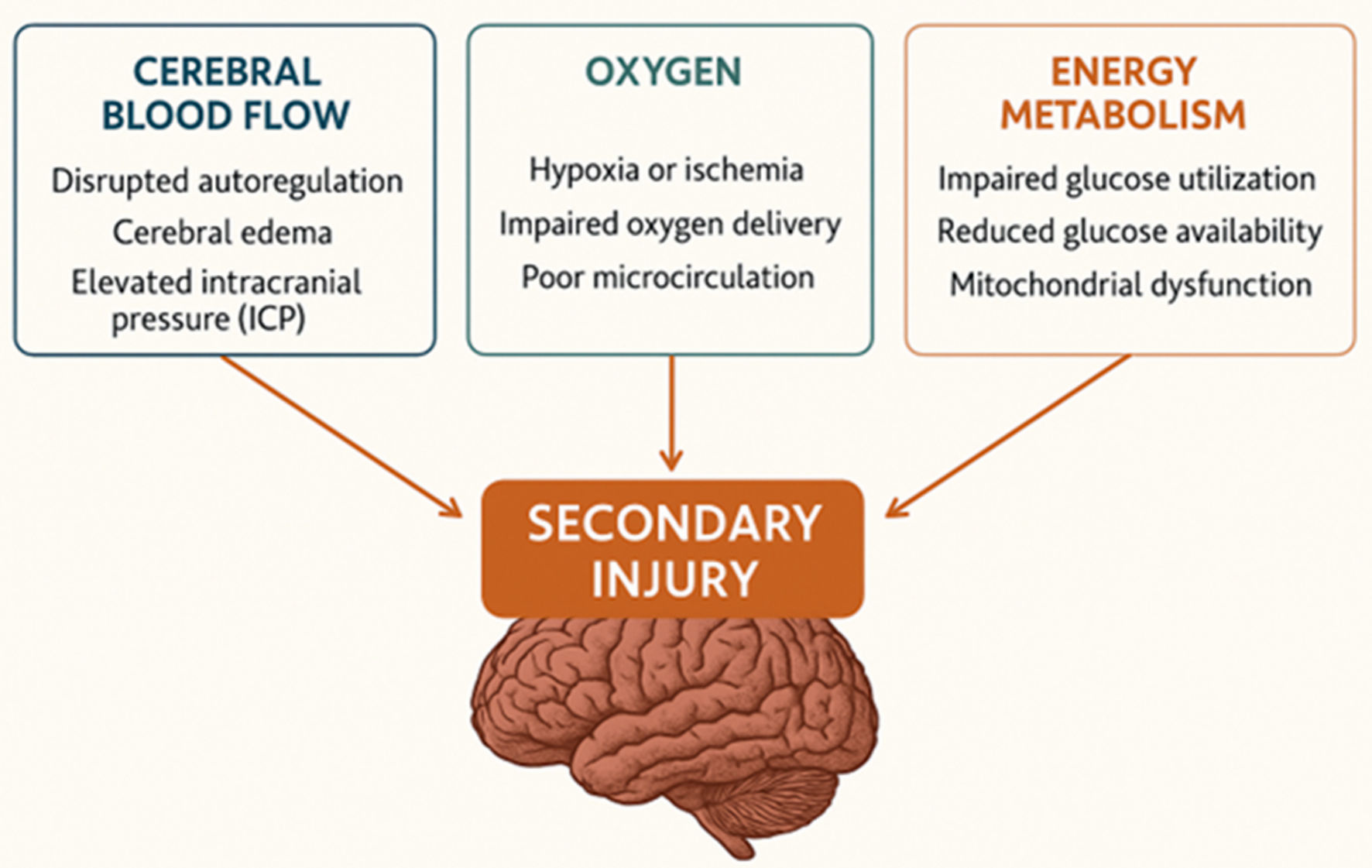 Click for large image | Figure 1. Secondary brain injury. |
Pathophysiology of TBI
The pathophysiology of TBI follows a sequential progression. Trauma initially results in a primary brain injury and triggers an inflammatory response. This is followed by cerebral swelling (edema) and increased ICP, which may ultimately lead to secondary brain injury.
Areas of the brain typically affected by TBI
Figure 2 illustrates the major brain regions and their functions that are commonly affected by traumatic brain injury.
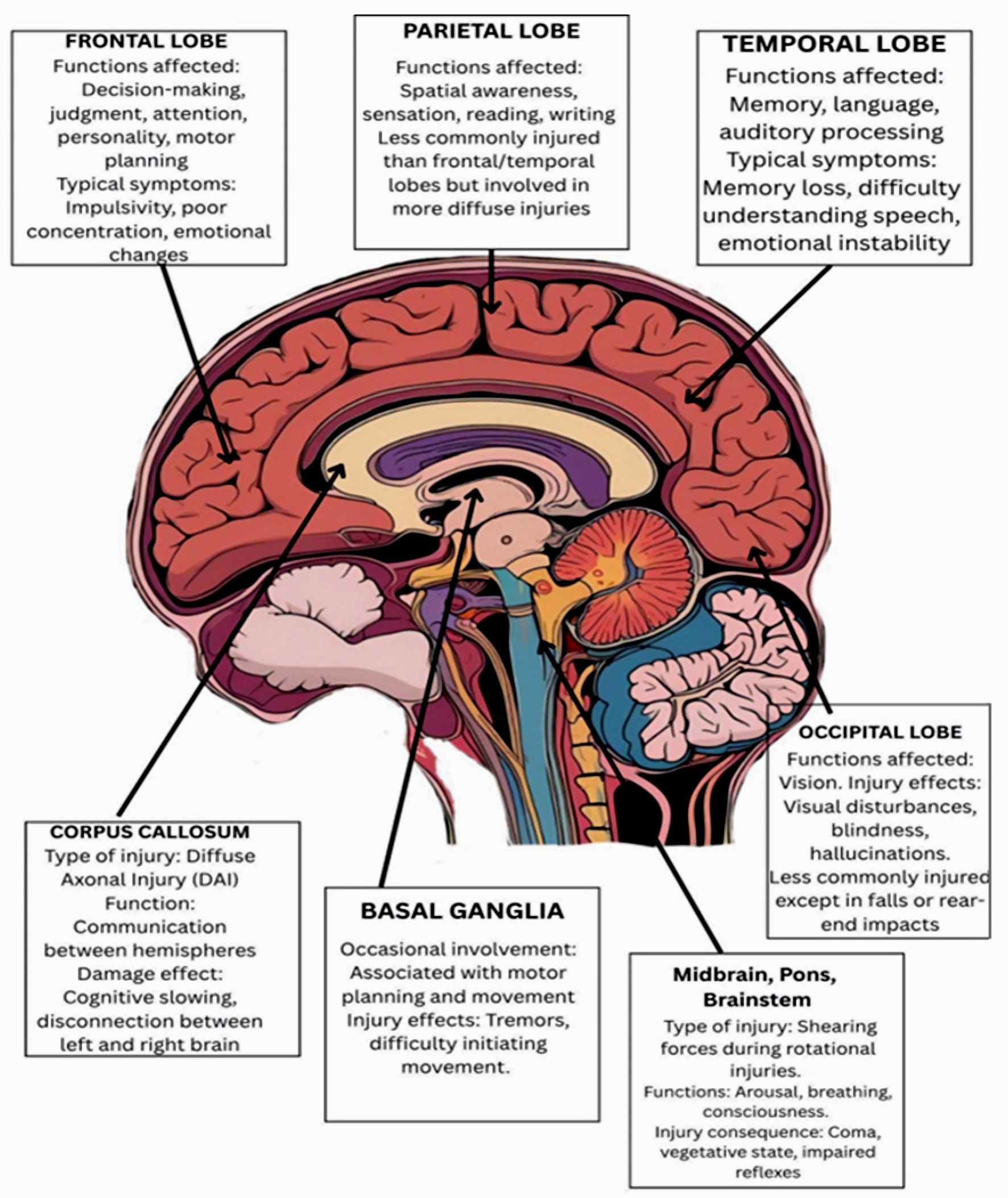 Click for large image | Figure 2. Major brain regions and their functions commonly affected by traumatic brain injury. |
| Impact of TBI on Personality Changes | ▴Top |
A person’s emotional and social functioning may be impacted by the substantial behavioral and personality changes that can result from TBI. These alterations, which result from the injury’s physiological disturbances of brain function, are frequently intricate and multidimensional [26].
There are many things that can make your personality change after a TBI. These may be pre-injury, injury-related, or post-injury elements. Individuals at greater risk are those who had an abnormal personality prior to the injury. People with abnormal personalities, such as mood disorder, anxiety and depression, or antisocial personality disorder characterized by impulsivity, aggression and sensation seeking, are more susceptible. Lower educational attainment is also associated with increased risk and may be considered a measure of cognitive function [27]. A history of substance uses disorders, including alcohol and drug use, is a significant risk factor for both TBI and subsequent personality changes [28].
The severity of the brain injury and where it is located will matter. A more severe TBI is more likely to impair personality if it includes damage to the frontal lobe or temporal lobes. The frontal lobe plays an important role in emotional control [29].
Following injury, the post-injury factors such as poor psychosocial support, disconnection from family, difficulties at work, lack of vocational rehabilitation and limited access to recovery services may further increase the likelihood of personality change [28]. Furthermore, having other problems like secondary attention-deficit/hyperactivity disorder (ADHD) can contribute to persistent personality changes, especially in kids with severe TBI [30].
TBI can cause a variety of personality changes by harming certain brain regions in charge of emotions, behavior, and social interactions. The degree and type of these alterations are largely determined by the location and severity of the damage. For example, impulsivity and emotional dysregulation are often linked to frontal lobe lesions [31], although social cognition and empathy may be impacted by injury to other regions, such as the orbitofrontal cortex (OFC). This area contributes to empathy and helps regulate impulsive behavior. If it is destroyed, the person may find it difficult to sympathize with others and may act more recklessly. However, changes in neuroticism are linked to lesions in the frontal and temporal regions. Higher executive activities, such as planning, thinking, problem solving, and emotional control, typically take place in the frontal lobe. Additionally, the temporal lobes are crucial for language and affect/emotion processing [32]. For example, 59.1% of patients with brain injury had personality changes, primarily in neuroticism, extraversion, and conscientiousness. Neuroticism changes were specifically linked to frontal or temporal lobe lesions, and changes in patient agreeableness were linked to lower emotional role limitations, personality changes in patients did not correlate with increased distress or decreased health-related quality of life [33].
In a study investigating personality changes 6 to 24 months after TBI, approximately 13% of participants experienced personality changes between 6 and 12 months post-TBI, and 12% in the second year. The personality changes were consistently predicted by the severity of the injury, and that frontal lobe white matter lesions were significantly associated with personality changes in the second year following the injury, while lesions of the superior frontal gyrus were linked to personality changes between 6 and 12 months after the injury [30].
The first case was reported in 1848, when 25-year-old railroad foreman Phineas Gage had a brain injury when a tamping iron was forced through his skull and into his frontal lobes. Before the accident, Gage was described as responsible and well-adjusted. But after his injury, he became a different man. After his injury, he became impulsive, irreverent, and socially inappropriate, showing a marked inability to plan, and a lack of respect for social conventions. This very dramatic personality change, first reported by his physician Dr. John Harlow, gave the first clear evidence that the frontal lobes—particularly the prefrontal cortex—are related to personality, social behavior, and executive functions. Gage’s case remains a landmark in neuroscience, providing evidence that the frontal lobes—particularly the prefrontal cortex—are related to personality, social behavior, and executive functions [34].
Individuals with TBI may experience a range of personality changes, including emotional dysregulation, loss of empathy, social behavior issues, aggression, apathy and loss of interest. Explicitly, many patients have elevated emotional reactions, including abrupt mood changes, irritation, and aggression. Inappropriate emotional displays, such as laughing when depressed, are another prominent sign of emotional lability. Decreased empathy is another obvious shift. This apathy, which may be more noticeable in men, might show itself as a disregard for other people’s needs or feelings [35]. Additionally, individuals with TBI may develop difficulties in interpreting social cues. Thus, they may exhibit poor social judgment and make improper remarks or behave inappropriately. This involves impetuous actions like saying hurtful things or acting in ways that are indecent. Additionally, a noted lack of emotional self-control can lead to impulsive aggressiveness. Changes in patients’ emotional states can cause them to react excessively to small provocations. Furthermore, some people may exhibit indifference or a lack of interest in things they used to enjoy, which might be mistaken for an introverted personality change [31].
Diving into details, first, impaired emotional regulation can be a serious consequence of TBI, restricting people to regulate their emotions in the right way. This situation can happen in many different ways, but usually it is the reason for many serious implications such as emotional difficulties in relationships and overall quality of life. This emotional turmoil mainly originates from the ruin of certain cerebral zones regulating mood, e.g., the prefrontal cortex and the limbic system. This issue could make the neural pathways, which aid in thinking and leading our life, disrupted [33]. Notably, patients may experience emotional lability, characterized by rapid and intense mood swings, often without an identifiable trigger [26]. Increased irritability is also common; this is displayed by people who find it easier to get irritated in general than by people around them, resulting in frequent outbursts and social conflicts [35]. Not to forget, anxiety and depression are observed. Exaggerated emotional response, apathy, and disengagement are also reported at this level [32].
Second, cognitive impairment may occur after TBI. People who have TBI frequently struggle to maintain focus and attention. This may make it difficult to follow discussions, finish assignments, and stay focused on activities. Both anterograde memory impairment (difficulty creating new memories) and retrograde memory impairment (loss of pre-existing memories) are notably common memory disorders. According to studies, episodic memory is commonly compromised, which impacts the recall of knowledge or events that occurred before the injury. Additionally, planning, problem-solving, language skills, and decision-making are examples of executive activities that are frequently impaired. People may find it difficult to efficiently manage their time, understand speech or even find words, organize their responsibilities, and control their conduct in social settings [33]. These impaired social skills may also be due to slower processing rates [36].
Impulse control is governed by the gyrus rectus and OFC. Damage to these areas from TBI interferes with the brain’s “braking mechanism,” which results in uncontrollable, impulsive actions [35]. In rodent models, impulsive decision-making is chronically increased by bilateral frontal injuries, even mild ones. Furthermore, impulsive behaviors after TBI are correlated with elevated levels of interleukin (IL)-12 in the frontal cortex, indicating that inflammatory pathways play a role in impulsivity [37].
Furthermore, TBI can profoundly impact an individual’s sense of self and identity, leading to feelings of disconnection from one’s previous self and uncertainty about the future. Survivors may have trouble remembering things, identifying people they know, or carrying out activities that were formerly effortless, including working, cooking, or playing sports. Gaps in autobiographical memory can also be noted. Plus, self-awareness issues are prevalent, especially in the early phases of recovery, and they can lead to bad choices or impractical objectives, which can lower motivation and jeopardize safety. TBI patients may become unable to track their performance and adjust their perception of their capabilities [36].
Borrowed identity syndrome can also be a consequence of TBI. Pachalska et al reported the case of a physician who suffered severe TBI with focal injuries to the right frontal and temporal areas, leading to significant and evolving disturbances in personal identity. The patient experienced a loss of autobiographical memory, impaired self-image, and diminished emotional connections to family. Over time, he exhibited behaviors such as borrowing identities from others, Capgras syndrome, and delusions, highlighting the complex interplay between brain injury, memory, and the construction of self [36].
A noteworthy case is a 30-year-old man, referred to as Patient 2410 in the study, who underwent surgery for a brain aneurysm and then demonstrated positive personality changes. Before the injury, the man was short-tempered, quick to anger, and generally “mopey.” He became more laid-back after his injury and started laughing and joking more and was called “more passive.” MRI revealed that individuals showing any personality improvements were more likely to have damage in the most frontal regions of the brain, most specifically, the bilateral frontal polar region, an area relevant for perspective-taking and decision-making (Fig. 3) [38, 39].
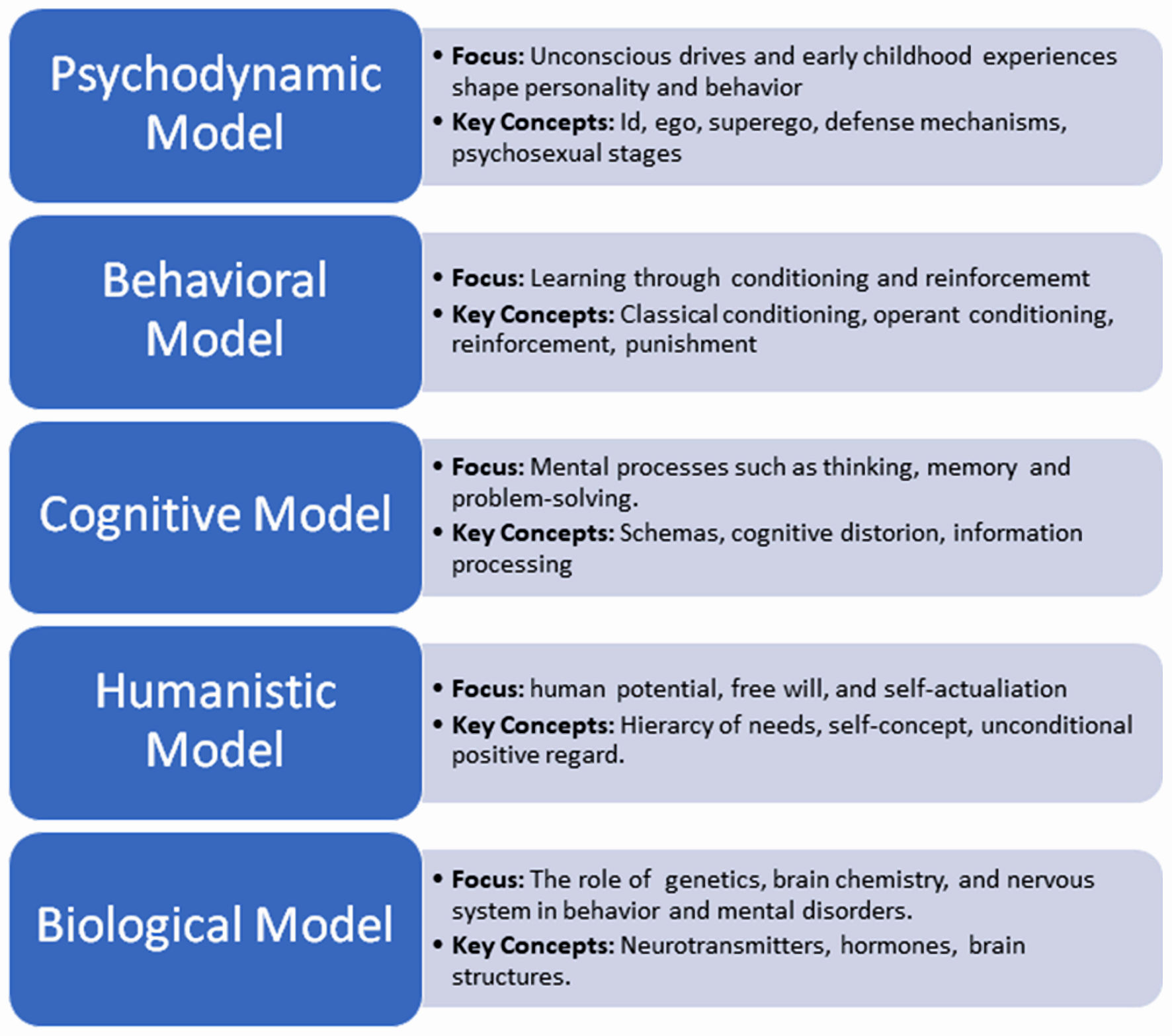 Click for large image | Figure 3. Overview of major psychological models, highlighting their focus areas and key concepts in understanding human behavior and mental processes [39]. |
| Impact of TBI on Behavioral Changes | ▴Top |
Cluster B personality disorders, specifically antisocial personality disorder and borderline personality disorder, have been positively associated with the history of TBI [40]. Furthermore, a positive correlation between TBI, worse executive functions, deteriorated emotional regulation, and higher impulsivity was reported by Betz et al (2024) [41]. The age of TBI injury seemed to be indispensable in determining which aspect of life is influenced the most. However, when trying to understand the neuropsychology behind domains affected, no changes in white matter microstructure were detected in TBI children compared to normal ones. This might be attributed to the fact that the children recruited in the study developed TBI 4 years before, and thus changes on MRI could have disappeared by the time of the study [41]. In addition, to better understand the impact of TBI on social behavior, adults with TBI reported that Facebook was a tool that helped them in self-disclosing compared to face-to-face interaction. On the contrary, this social compensation hypothesis was partially proven, as TBI individuals were not able to express support, interest, or any other maintenance social behavior while using this platform [42]. Hence, although social medial platforms assisted in combating social isolation in individuals with TBI, many key aspects of social behavior remain impaired. Behavioral changes, including aggressive and violent behavior were increased in individuals with TBI [27]. Supporting the relationship between aggression and TBI, a study in Denmark reported a suicide rate of 21 per 100,000 between 1980 and 2014, compared to almost double that rate (41 per 100,000) among individuals with TBI [43].
Alterations in dopaminergic pathways after TBI have been implicated in the development of mood and anxiety disorders, and changes in dopamine neurotransmission after injury are associated with cognitive and behavioral impairments in patients [44].
There is a long-standing idea of excitatory–inhibitory disruption following TBI, and the second neurological pathway among the most common to be affected is GABAergic neurotransmission. In diffuse TBI conditions, tensile forces applied to the brain can cause DAI in both glutamatergic and GABAergic neurons. The DAI due to chronic TBI may correspond to a long-term positive feedback loop for glutamatergic signaling. This uncontrolled increase in glutamate release can potentially lead to glutamate excitotoxicity, a characteristic outcome of TBI. The alterations in GABA concentrations have been correlated to various neuropsychiatric disorders. This suggests that novel methods involving spatial and temporal delivery of GABA could help in restoring cognitive reserve and improve behavioral outcomes in TBI survivors [45].
TBI is a challenging disease to treat as it varies according to the site of lesion and its severity based on individualized conditions. Therefore, its treatment requires innovative compensatory methods for neurobehavioral recovery.
In a report on a 27-year-old male with TBI aimed to decipher the reason of disinhibition and violent behavior, diffusion tensor tractography (DTT) revealed impairment and decrease in the connections between amygdala and OFC in both hemispheres in addition to injuries of both anterior cingulums in anterior cingulate cortex (ACC) [46].
In a 47-year-old man with post-TBI sequelae, utilizing progressive muscle relaxation (PMR), meditation, and mental-based strategies made the patient better perform motor tasks, communication, hobbies, physical and psychosocial functions [47]. Furthermore, adopting holistic rehabilitation, rather than just physical recovery, can lead to improvements in psychological and social quality of life. Hence, in rehabilitation, it is indispensable to tackle the domains considered essential by the TBI patients, such as methods of improving self-care, family relationships and understanding, in addition to performing spiritual practices [48]. Educational level, income, and cause of TBI, all appeared to affect the family’s knowledge of TBI and their attitude towards TBI patients. Thus, initiatives that target knowledge gaps might help family members better manage TBI outcomes and provide sufficient care and support [49].
| Psychiatric Comorbidities and TBI | ▴Top |
TBI increases the risk of developing mental diseases such as depression, anxiety, and post-traumatic stress disorder (PTSD). According to studies, 14% of TBI patients have anxiety disorders, 25% have depressive disorders, and 7% have comorbid anxiety and depression [50]. It was reported that 40% of TBI patients had two or more psychiatric conditions, meaning that the prevalence of psychiatric problems following TBI is higher than those in the general population. The two most common mental health conditions—major depressive disorder and PTSD—typically appear during the first year after an accident. Although unusual illnesses can develop following TBI, people who had a history of mental illness before the injury are at a higher risk. The relationship between TBI and substance use disorders (SUDs) is complex and reciprocal. Both substances use and TBI may increase the chance of developing SUDs [51]. According to recent studies, factors influencing this connection include sex differences, age at injury, and injury severity [52]. TBI can cause mild cognitive and executive function impairments that can make a person more susceptible to substance misuse. Various mechanisms have been hypothesized to explain this link, including alterations in brain networks, damage-associated neuroplasticity, and chronic neuroimmune signaling changes [53]. The methods used to treat these disorders include neuromodulation techniques, medication, and cognitive-behavioral therapy [54]. Stronger empirical evidence is needed to guide therapy, as the intricacy of post-TBI psychiatric disorders makes treatment challenging [55]. To better understand underlying mechanisms and provide person-centered care for TBI patients with psychiatric comorbidities, future research should focus on developing novel treatment strategies and conducting pragmatic trials [54]. It is crucial to provide integrated mental health care to patients with TBI who also have concurrent illnesses. Numerous levels and types of integrated treatment, including micro-and meso-level clinical and service integration, are already available for TBI and mental health concerns. However, issues including fragmented treatment and ignorance of TBI-related cognitive impairments persist. Experts say that improving outcomes can be achieved by educating medical staff, forming interdisciplinary teams, and providing patients with cognitive accommodation [56].
Mind–body–based rehabilitation approaches such as progressive muscle relaxation and meditation have shown potential benefit in TBI-related tremor management [47].
The neurological consequences ultimately affect the quality of life in TBI survivors. Moreover, dopamine may be important in neuroplasticity, neural sprouting, and synaptogenesis corresponding to the use of dopaminergic genes in the treatment of cognitive deficits post-TBI [57]. Treble-Barna et al reported such neurobehavioral recuperation in child survivors of TBI [58].
Neuroplasticity is a process that takes place after a neuronal injury, which is defined as structural and functional changes to restore the brain’s activity in response to an external or internal trauma to the brain [59]. Such an ability to form new neural connections within the brain after primary diffuse injury holds crucial importance in TBI.
There are various neuroimaging modalities used to monitor neuroplasticity after TBI. The most common ones include positron emission tomography (PET), functional magnetic resonance imaging (fMRI), diffusion tensor imaging (DTI) and transcranial magnetic stimulation (TMS). These modalities help detect the white matter changes after brain injury [60].
| Rehabilitation and Interventions for Personality and Behavioral Changes | ▴Top |
TBI may induce extensive alterations in behavior and personality, typically manifesting in the form of aggression, irritability, apathy, impulsivity, and emotional dysregulation. These consequences necessitate special rehabilitation interventions involving psychological, cognitive, pharmacological, and social domains for enhanced recovery and reintegration. Behavior therapy is aimed at changing maladaptive behavior via reinforcement, modeling, and environmental structuring. Cognitive rehabilitation addresses executive functioning deficits, attentional deficits, and memory deficits that are prevalent following TBI, and facilitates enhanced emotional regulation and social behavior [61]. Both these approaches improve self-awareness and self-control when used together. Cognitive behavioral therapy (CBT) is one of the most helpful treatments for treating post-TBI emotional and behavioral dysregulation. It promotes emotional control, diminishes aggression, and enhances interpersonal relationships [62]. Other treatments comprise anger management training, mindfulness-based cognitive therapy, social skills training, and acceptance and commitment therapy (ACT), with customization to neuropsychological profiles [63]. Pharmacologic interventions are usually employed adjunctively with treatment to stabilize mood and manage severe behavioral symptoms. Drugs have to be selected with care because of changed neurochemistry and heightened sensitivity following injury [64]. The classes of drugs used include antipsychotics, antidepressants and mood stabilizers. Selective serotonin reuptake inhibitors (SSRIs), e.g., sertraline, are useful for the treatment of depression and irritability [65]. For anger, beta-blockers such as propranolol and mood stabilizers like valproic acid have been found helpful [66]. Atypical antipsychotics such as quetiapine and risperidone may be used occasionally for extreme behavioral dysregulation but need to be monitored for possible side effects [67]. Recovery from personality and behavioral changes is usually slow and based on the severity and site of injury. Recovery can go on for years after injury, especially with early treatment. Some personality changes are chronic and require long-term management [68]. Several factors influence recovery, including age at injury, pre-injury personality, injury severity, access to rehabilitation, and the presence of psychiatric comorbidities [69]. Family support, motivation, and helpful community also play effective part in adaptive outcomes. Family support largely influences outcomes in behavior. The education of families regarding TBI-induced behavioral changes can improve coping and enhance treatment adherence by the patient. Social support has been associated with increased emotional stability and functional independence [70]. Caregivers provide daily care and emotional support. Involvement in planning for rehabilitation promotes continuity of care. The burden on caregivers is high but needs psychosocial intervention and respite services. Community-based services and networks can help alleviate loneliness and improve recovery in the long term [71]. In summary, personality rehabilitation and behavioral changes after TBI need a multimodal and patient-focused strategy. Successful management relies on personalized therapy, proper pharmacological intervention, and intense family and social participation.
| Challenges in Clinical Research and Clinical Practice | ▴Top |
The post-TBI results are very variable, and more effort is needed to determine who is bound to heal or show chronic disability. An interaction of complex determinants such as severity of injuries, demographics, social economic and socio-economic factors, genetic and molecular signatures, comorbid conditions and healthcare disparities facilitate such heterogeneity [72]. Notable among these factors that are always linked with poor prognosis include advanced age, low GCS scores, and high injury severity. The number and severity of cognitive, psychic, and bodily sequelae after TBI do not decline: slightly more than half of patients are still struggling with memory problems, fatigue, and mood swings 6 months after their injury [73]. GCS scores < 8 are related to a fatality rate of 30–40 % with survivors being severely impaired, especially elderly adults [74]. Also, older age presents a negative effect on recovery patterns, probably because of underlying health problems and reduced physiological strength [73]. Moreover, repetitive mild TBIs, which are prevalent in the cases of athletes, have a twofold increased risk of long-term neurological complications compared to one event [75]. Genetic influences on TBI outcomes are also evident. The single nucleotide polymorphisms, other than APOE, have been found to affect patient-oriented recovery, meaning that the genetic basis of post-injury adaptation are heterogeneous [76]. Variants such as APOe4 increase the risk of poor performance in moderate-to-severe TBI by 20–30% [77]. Collectively, these results emphasize the vast number of predictors that determine the outcomes of TBI and the requirement of the personalized multidisciplinary rehabilitation and long-term care.
Besides genetic factors, non-biological factors such as race or ethnicity, access to healthcare, comorbidities, and social supports also moderate TBI resilience. People from minority groups or those without full insurance often face delays in getting care. These delays can lead to worse recovery and health outcomes [78].
TBI is a complex issue that presents a serious challenge to clinicians and scientists. Published literature, especially randomized controlled trials and surgery research, is highly skewed by limited-time reviews (often weeks or months), and cohort samples are relatively small, especially in severe TBI, where studies rarely include more than 100 participants. Moreover, few of those trials receive the classification of being at low risk of bias in the following areas, including randomization method or allocation concealment [79]. At the same time, the research of biomarkers faces certain barriers due to the patient presentation variability. Time delay after injury, systematic inflammatory condition, and accelerated heredity are variables that impact serum levels of biomarkers related to TBI [80]. The combination of these methodological, biological, and translational limitations slows down the TBI research. They will require international, multisite sample groups, complex methods, and increased collaboration to combine efforts between disciplines, to practice and improve clinical features and develop the field.
There is a lack of longitudinal evidence, which limits the knowledge of the sequelae of TBI several years after injury. There are limited global, standardized, and strictly validated measures for assessing long-term outcomes. For instance, moderate-to-severe TBI in veterans more than doubles (60%) the risks of dementia, but the nature of milder TBI is currently poorly understood, and only male veterans were included in the sample [81]. Furthermore, few studies have examined mild TBI or non-military groups with follow-up periods longer than 5 to 10 years [82, 83]. These restrictions make it hard to tell whether results improve or worsen over decades. Less than 10% of all TBI studies investigate participants after a period of more than 12 months, which leaves large knowledge gaps regarding progressive brain decline [79]. Two recent markers, neurofilament light (NfL) and glial fibrillary acidic protein (GFAP), allow doctors to monitor the persistent brain damage progression and inform prognosis. However, such indicators are primarily experimental, and they are not widely used in everyday long-term care [84, 85]. There are other sub-populations that are not adequately represented in longitudinal studies such as older adults, children and those with repeated or mild TBI [86].
TBI raises many ethical questions, making it challenging to manage patients and conduct clinical research. Since a large proportion of patients lose the possibility to make treatment choice, family members take this role, which can lead to a conflict situation on the most proper choice. In addition, rehabilitation services are extremely unequal: poorer citizens tend to get less care than those with better-resourced health systems. Doctors often focus on life-saving interventions, but relatives focus on the quality of life, and descriptions of miraculous improvement stories of patients may create false expectations and unrealistic outcomes [87]. Although artificial intelligence (AI) in TBI provides tools in predicting mortality, functional outcomes, and personalized rehabilitation strategies for TBI patients [88], it raises concerns about data privacy, algorithmic bias, and transparency [89]. Hence, there is a need to formulate strong ethical standards that can incorporate perspectives from multi modalities.
Obtaining informed consent in severe TBI patients is challenging, as most cannot speak for themselves. Family usually has the duty to cover this aspect, but the emotional stress of attending to a critically ill family member may affect its ability to make sound decisions. According to Van Dijck et al (2020) [90], such contextual factors cause delays in up to 83% of cases, affecting treatment efficacy. In emergencies, doctors may need to act quickly before getting full consent. If local laws allow, they can use deferred consent, meaning they treat the patient first and get consent later [90, 91]. However, regulatory authorities—especially in Europe—do not allow informed consent to be waived to conduct research activities, thus delaying interventions compared to more liberal policies elsewhere [90]. These issues are even more challenging in children, especially when parents are not present in time to give consent during critical stages of treatment. That is why flexible exceptions to the usual informed consent rules are very important in emergencies [92].
| Conclusions | ▴Top |
TBI is a complex clinical and societal condition with consequences that extend well beyond the initial injury. The emphasis on initiating interventions for motor and cognitive impairments has been the focus of most TBI studies. However, this review emphasizes the equally debilitating impacts of personality and behavioral changes, and recognizes that changes in emotional regulation, impulse control, empathy, and identity can result in negative social function and relationships and overall quality of life. The neuropsychiatric consequences of TBI are influenced by the location of brain damage, severity of injury, and pre-injury vulnerabilities, along with psychosocial context and access to after-care rehabilitation.
There has been an increasing awareness that the frontiers of personality and behavioral outcomes of TBI have been overlooked, both in research and clinical practice. Successful rehabilitation is facilitated by an integrated interdisciplinary approach, which addresses neuropsychological assessment, planned individualized therapy, pharmacological management, and community/family involvement. Advances in neuroimaging, conceptualizations of neuroplasticity, and characterizations of biomarkers are essential to better address personalized approaches to care, but research is still trying to address methodological and evidence thresholds, socio-political care inequities, and ethical issues surrounding consent and comprehensiveness of follow-ups.
Future efforts should be focused on addressing the limitations identified above in a collaborative, person-centered manner, which will be integral to improving outcomes and quality of life for individuals with TBI.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Author Contributions
Muhammad Saeed: conceptualization, investigations, methodology, supervision, writing original manuscript, manuscript review and editing; Sumaiyya Syeda: conceptualization, investigations, methodology, supervision, writing original manuscript, manuscript review and editing; Muhammad Umar Ahsan: investigations, methodology, writing original draft, conceptualization, manuscript review, formal analysis; Maha Ahmed: investigations, methodology, writing original draft; Manognya Gaddam: investigations, methodology, writing original draft; Lea Nohra: investigations, methodology, writing original draft; Sourav Paul: conceptualization, manuscript review and editing, formal analysis; Kanchan Chaudhary: methodology, writing original draft; Muniba Syed: investigations, writing original draft; Sara Ajami: conceptualization, manuscript review and editing, formal analysis; Rabbea Ali: methodology, writing original draft, conceptualization, manuscript review; Aghna Iman: investigations, methodology, writing original draft.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Slot RER, Helbok R, van der Jagt M. Update on traumatic brain injury in the ICU. Curr Opin Anaesthesiol. 2025;38(2):93-99.
doi pubmed - Parikh S, Koch M, Narayan RK. Traumatic brain injury. Int Anesthesiol Clin. 2007;45(3):119-135.
doi pubmed - Chauhan NB. Chronic neurodegenerative consequences of traumatic brain injury. Restor Neurol Neurosci. 2014;32(2):337-365.
doi pubmed - Gardner RC, Bahorik A, Kornblith ES, Allen IE, Plassman BL, Yaffe K. Systematic review, meta-analysis, and population attributable risk of dementia associated with traumatic brain injury in civilians and veterans. J Neurotrauma. 2023;40(7-8):620-634.
doi pubmed - Al-Rubaie A. Traumatic brain injury and dementia: mechanisms, risk stratification, and clinical management. J Clin Neurol. 2025;21(4):265-276.
doi pubmed - Ginsburg JC, Huff JS. Closed Head Trauma. 2020. https://www.semanticscholar.org/paper/ea696704a396ecc5a1cc97b68ab41e3f60bdf8a2.
- Malec JF, Brown AW, Leibson CL, Flaada JT, Mandrekar JN, Diehl NN, Perkins PK. The mayo classification system for traumatic brain injury severity. J Neurotrauma. 2007;24(9):1417-1424.
doi pubmed - Esselman PC, Uomoto JM. Classification of the spectrum of mild traumatic brain injury. Brain Inj. 1995;9(4):417-424.
doi pubmed - Yan J, Wang C, Sun B. Global, regional, and national burdens of traumatic brain injury from 1990 to 2021. Front Public Health. 2025;13:1556147.
doi pubmed - Guan B, Anderson DB, Chen L, Feng S, Zhou H. Global, regional and national burden of traumatic brain injury and spinal cord injury, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ Open. 2023;13(10):e075049.
doi pubmed - Khan F, Baguley IJ, Cameron ID. 4: Rehabilitation after traumatic brain injury. Med J Aust. 2003;178(6):290-295.
doi pubmed - McKay SM. Personality and behavior changes subsequent to traumatic brain injury: a review of the literature. Int J Emerg Ment Health Hum Resilience. 2015;17(2):469-474.
doi - Buzan RD, Kupfer J, Eastridge D, Lema-Hincapie A. Philosophy of mind: coming to terms with traumatic brain injury. NeuroRehabilitation. 2014;34(4):601-611.
doi pubmed - Azouvi P, Arnould A, Dromer E, Vallat-Azouvi C. Neuropsychology of traumatic brain injury: An expert overview. Rev Neurol (Paris). 2017;173(7-8):461-472.
doi pubmed - Russo L, Kazmi A, Ahmed N. Current management and future challenges in the management of severe traumatic brain injury. Medicina (Kaunas). 2025;61(4):738.
doi pubmed - Hyder AA, Wunderlich CA, Puvanachandra P, Gururaj G, Kobusingye OC. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007;22(5):341-353.
pubmed - Ogonah MGT, Botchway S, Yu R, Schofield PW, Fazel S. An umbrella review of health outcomes following traumatic brain injury. Nat Ment Health. 2025;3(1):83-91.
doi pubmed - Andriessen TM, Jacobs B, Vos PE. Clinical characteristics and pathophysiological mechanisms of focal and diffuse traumatic brain injury. J Cell Mol Med. 2010;14(10):2381-2392.
doi pubmed - Pudenz RH, Shelden CH. The lucite calvarium; a method for direct observation of the brain; cranial trauma and brain movement. J Neurosurg. 1946;3(6):487-505.
doi pubmed - Jang SH, Cho MJ. Role of diffusion tensor imaging in the diagnosis of traumatic axonal injury in individual patients with a concussion or mild traumatic brain injury: a mini-review. Diagnostics (Basel). 2022;12(7):1580.
doi pubmed - Galgano M, Toshkezi G, Qiu X, Russell T, Chin L, Zhao LR. Traumatic brain injury: current treatment strategies and future endeavors. Cell Transplant. 2017;26(7):1118-1130.
doi pubmed - Schimmel SJ, Acosta S, Lozano D. Neuroinflammation in traumatic brain injury: A chronic response to an acute injury. Brain Circ. 2017;3(3):135-142.
doi pubmed - Sharma Y, Popescu A, Horwood C, Hakendorf P, Thompson C. Relationship between vitamin C deficiency and cognitive impairment in older hospitalised patients: a cross-sectional study. Antioxidants (Basel). 2022;11(3):463.
doi pubmed - https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2022.85570110.3389/fimmu.2022.855701.
- Greene C, Connolly R, Brennan D, Laffan A, O'Keeffe E, Zaporojan L, O'Callaghan J, et al. Blood-brain barrier disruption and sustained systemic inflammation in individuals with long COVID-associated cognitive impairment. Nat Neurosci. 2024;27(3):421-432.
doi pubmed - Hanna D, Priven S, Carroll N, Ekladios H, Fitzsimmons A. Psychosis and personality changes following traumatic brain injury. Cureus. 2024;16(11):e72849.
doi pubmed - Maresca G, Lo Buono V, Anselmo A, Cardile D, Formica C, Latella D, Quartarone A, et al. Traumatic brain injury and related antisocial behavioral outcomes: a systematic review. Medicina (Kaunas). 2023;59(8):1377.
doi pubmed - Bryant BR, Richey LN, Jahed S, Heinzerling A, Stevens DA, Pace BD, Tsai J, et al. Behavioral and emotional dyscontrol following traumatic brain injury: a systematic review of neuroimaging and electrophysiological correlates. J Acad Consult Liaison Psychiatry. 2022;63(6):579-598.
doi pubmed - Yeates KO, Max JE, Narad ME. Advances in understanding the association between pediatric traumatic brain injury and attention-deficit/hyperactivity disorder. JAMA Pediatr. 2021;175(10):1001-1003.
doi pubmed - Max JE, Levin HS, Schachar RJ, Landis J, Saunders AE, Ewing-Cobbs L, Chapman SB, et al. Predictors of personality change due to traumatic brain injury in children and adolescents six to twenty-four months after injury. J Neuropsychiatry Clin Neurosci. 2006;18(1):21-32.
doi pubmed - Weis CN, Webb EK, deRoon-Cassini TA, Larson CL. Emotion dysregulation following trauma: shared neurocircuitry of traumatic brain injury and trauma-related psychiatric disorders. Biol Psychiatry. 2022;91(5):470-477.
doi pubmed - Bryant AM, Rose NB, Temkin NR, Barber JK, Manley GT, McCrea MA, Nelson LD, et al. Profiles of cognitive functioning at 6 months after traumatic brain injury among patients in level I trauma centers: A TRACK-TBI study. JAMA Netw Open. 2023;6(12):e2349118.
doi pubmed - https://www.frontiersin.org/journals/behavioral-neuroscience/articles/10.3389/fnbeh.2024.1326115/full.
- Freitas VS, Rodrigues RAF, Gaspi FOG. Propriedades farmacologicas da Aloe vera (L.) Burm f. Rev Bras Plantas Med. 2014;16(2):299-307.
- Lee Y, Choi Y, Jeon J, Leigh JH, Kim DK, Oh BM. Impact of mild traumatic brain injury on health behaviors. Sci Rep. 2025;15(1):1585.
doi pubmed - Pachalska M, MacQueen BD, Kaczmarek BL, Wilk-Franczuk M, Herman-Sucharska I. A case of "borrowed identity syndrome" after severe traumatic brain injury. Med Sci Monit. 2011;17(2):CS18-28.
doi pubmed - Semanision K, Williams R, Moran E. et al. Psychosocial determinants conferring resilience after TBI: current understanding. Curr Phys Med Rehabil Rep. 2024;12:359-367.
doi - When personality changes from bad to good [Internet]. 2018 [cited Feb 9, 2025]. Available from: https://www.bbc.com/future/article/20180108-when-personality-changes-from-bad-to-good.
- 2.3 Psychological models - fundamentals of psychological disorders [Internet]. [cited Feb 9, 2025]. Available from: https://opentext.wsu.edu/fundamentalsofpsychologicaldisorders/chapter/2-3-psychological-models/.
- Moley JP, Norman JL, Coccaro EF. Personality disorder and mild traumatic brain injury. Personal Ment Health. 2022;16(4):331-337.
doi pubmed - Betz AK, Cetin-Karayumak S, Bonke EM, Seitz-Holland J, Zhang F, Pieper S, O'Donnell LJ, et al. Executive functioning, behavior, and white matter microstructure in the chronic phase after pediatric mild traumatic brain injury: results from the adolescent brain cognitive development study. Psychol Med. 2024;54(9):2133-2143.
doi pubmed - Toma CL, Hwang J, Kakonge L, Morrow EL, Turkstra LS, Mutlu B, Duff MC. Does Facebook Use Provide Social Benefits to Adults with Traumatic Brain Injury? Cyberpsychol Behav Soc Netw. 2024;27(3):214-220.
doi pubmed - Madsen T, Erlangsen A, Orlovska S, Mofaddy R, Nordentoft M, Benros ME. Association between traumatic brain injury and risk of suicide. JAMA. 2018;320(6):580-588.
doi pubmed - Luo H, Liu N, Lin C. Dopamine enhances recovery after traumatic brain injury through ubiquitylation and autophagic degradation of RIPK1. Cell Commun Signal. 2024;22(1):134.
doi pubmed - Witkin JM, Shafique H, Cerne R, Smith JL, Marini AM, Lipsky RH, Delery E. Mechanistic and therapeutic relationships of traumatic brain injury and gamma-amino-butyric acid (GABA). Pharmacol Ther. 2024;256:108609.
doi pubmed - Jang SH, Kwon HG. Severe disinhibition due to injuries of neural tracts related to emotion circuit in a patient with traumatic brain injury: A case report. Medicine (Baltimore). 2017;96(52):e9493.
doi pubmed - Campbell AH, Barta K, Sawtelle M, Walters A. Progressive muscle relaxation, meditation, and mental practice-based interventions for the treatment of tremor after traumatic brain injury. Physiother Theory Pract. 2024;40(10):2441-2457.
doi pubmed - Miller LR, Divers R, Reed C, Cherry J, Patrick A, Calamia M. Value-consistent rehabilitation is associated with long-term psychological flexibility and quality of life after traumatic brain injury. Neuropsychol Rehabil. 2024;34(7):955-973.
doi pubmed - He J, Chen Z, Zhang J, Liu X. Knowledge and attitudes toward mild traumatic brain injury among patients and family members. Front Public Health. 2024;12:1349169.
doi pubmed - Sudhakar SK, Sridhar S, Char S, Pandya K, Mehta K. Prevalence of comorbidities post mild traumatic brain injuries: a traumatic brain injury model systems study. Front Hum Neurosci. 2023;17:1158483.
doi pubmed - Knapp CP, Papadopoulos E, Loweth JA, Raghupathi R, Floresco SB, Waterhouse BD, Navarra RL. Perturbations in risk/reward decision making and frontal cortical catecholamine regulation induced by mild traumatic brain injury. Behav Brain Res. 2024;467:115002.
doi pubmed - Merkel SF, Cannella LA, Razmpour R, Lutton E, Raghupathi R, Rawls SM, Ramirez SH. Factors affecting increased risk for substance use disorders following traumatic brain injury: What we can learn from animal models. Neurosci Biobehav Rev. 2017;77:209-218.
doi pubmed - Olsen CM, Corrigan JD. Does traumatic brain injury cause risky substance use or substance use disorder? Biol Psychiatry. 2022;91(5):421-437.
doi pubmed - Fann JR, Quinn DK, Hart T. Treatment of psychiatric problems after traumatic brain injury. Biol Psychiatry. 2022;91(5):508-521.
doi pubmed - Chan V, Toccalino D, Omar S, Shah R, Colantonio A. A systematic review on integrated care for traumatic brain injury, mental health, and substance use. PLoS One. 2022;17(3):e0264116.
doi pubmed - https://www.semanticscholar.org/paper/A-systematic-review-on-integrated-care-for-brain-Chan-Toccalino/2c21d80808d1aa3bb9e89e4dcb744246c299a77f.
- Richard SA. Elucidating the pivotal molecular mechanisms, therapeutic and neuroprotective effects of lithium in traumatic brain injury. Brain Behav. 2024;14(6):e3595.
doi pubmed - Treble-Barna A, Wade SL, Martin LJ, Pilipenko V, Yeates KO, Taylor HG, Kurowski BG. Influence of Dopamine-Related Genes on Neurobehavioral Recovery after Traumatic Brain Injury during Early Childhood. J Neurotrauma. 2017;34(11):1919-1931.
doi pubmed - Puderbaugh M, Emmady PD. Neuroplasticity. In: StatPearls. Treasure Island (FL) ineligible companies. 2026.
pubmed - Blasi V, Rapisarda L, Cacciatore DM, Palumbo E, Di Tella S, Borgnis F, Baglio F. Structural and functional neuroplasticity in music and dance-based rehabilitation: a systematic review. J Neurol. 2025;272(5):329.
doi pubmed - Julien A, Danet L, Loisel M, Brauge D, Pariente J, Peran P, Planton M. Update on the efficacy of cognitive rehabilitation after moderate to severe traumatic brain injury: a scoping review. Arch Phys Med Rehabil. 2023;104(2):315-330.
doi pubmed - Pepping N, Weinborn M, Pestell CF, Preece DA, Malkani M, Moore S, Gross JJ, et al. Improving emotion regulation ability after brain injury: a systematic review of targeted interventions. Neuropsychol Rehabil. 2025;35(6):1283-1323.
doi pubmed - MacKenzie HM, Flores-Sandoval C, Bateman EA, McIntyre A, Barua U, Mehta S, Bayley M, et al. Evidence-based review of randomized controlled trials of interventions for the management of behavioral issues in individuals with moderate to severe traumatic brain injury. J Head Trauma Rehabil. 2024;39(5):369-381.
doi pubmed - Neurobehavioral Guidelines Working Group, Warden DL, Gordon B, McAllister TW, Silver JM, Barth JT, Bruns J, et al. Guidelines for the pharmacologic treatment of neurobehavioral sequelae of traumatic brain injury. J Neurotrauma. 2006;23(10):1468-1501.
doi pubmed - SciSpace - Paper [Internet]. StatPearls Publishing; 2020 [cited Jul 17, 2025]. Selective serotonin reuptake inhibitors. Available from: https://scispace.com/papers/selective-serotonin-reuptake-inhibitors-4r99bw033r.
- Downar J, Lapenskie J, Kanji S, Watpool I, Haines J, Saeed U, Porteous R, et al. Propranolol as an anxiolytic to reduce the use of sedatives for critically ill adults receiving mechanical ventilation (PROACTIVE): an open-label randomized controlled trial. Crit Care Med. 2025;53(2):e257-e268.
doi pubmed - Hart S, Lannon M, Chen A, Martyniuk A, Sharma S, Engels PT. Beta blockers in traumatic brain injury: a systematic review and meta-analysis. Trauma Surg Acute Care Open. 2023;8(1):e001051.
doi pubmed - Personality and behavior changes subsequent to traumatic braininjury: a review of the literature. International Journal of Emergency Mental Health and Human Resilience. 2015;17(2):1-6.
- Parental factors associated with recovery after mild traumatic brain injury: a systematic review. Journal of Neurotrauma [Internet]. 2023 [cited Jul 17, 2025]; Available from: https://scispace.com/papers/parental-factors-associated-with-recovery-after-mild-2snvaflm.
- Lovstad M, Borgen IMH, Hauger SL, Kleffelgard I, Brunborg C, Roe C, Soberg HL, et al. Family member reported symptom burden, predictors of caregiver burden and treatment effects in a goal-oriented community-based randomized controlled trial in the chronic phase of traumatic brain injury. BMC Neurol. 2024;24(1):333.
doi pubmed - Rivera PA, Elliott TR, Berry JW, Grant JS. Problem-solving training for family caregivers of persons with traumatic brain injuries: a randomized controlled trial. Arch Phys Med Rehabil. 2008;89(5):931-941.
doi pubmed - Gao G, Wu X, Feng J, Hui J, Mao Q, Lecky F, Lingsma H, et al. Clinical characteristics and outcomes in patients with traumatic brain injury in China: a prospective, multicentre, longitudinal, observational study. Lancet Neurol. 2020;19(8):670-677.
doi pubmed - Maas AIR, Menon DK, Manley GT, Abrams M, Akerlund C, Andelic N, Aries M, et al. Traumatic brain injury: progress and challenges in prevention, clinical care, and research. Lancet Neurol. 2022;21(11):1004-1060.
doi pubmed - Steyerberg EW, Wiegers E, Sewalt C, Buki A, Citerio G, De Keyser V, Ercole A, et al. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: a European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019;18(10):923-934.
doi pubmed - Manley G, Gardner AJ, Schneider KJ, Guskiewicz KM, Bailes J, Cantu RC, Castellani RJ, et al. A systematic review of potential long-term effects of sport-related concussion. Br J Sports Med. 2017;51(12):969-977.
doi pubmed - Zeiler FA, McFadyen C, Newcombe VFJ, Synnot A, Donoghue EL, Ripatti S, Steyerberg EW, et al. Genetic influences on patient-oriented outcomes in traumatic brain injury: a living systematic review of non-apolipoprotein e single-nucleotide polymorphisms. J Neurotrauma. 2021;38(8):1107-1123.
doi pubmed - McFadyen CA, Zeiler FA, Newcombe V, Synnot A, Steyerberg E, Gruen RL, Rosand J, et al. Apolipoprotein E4 polymorphism and outcomes from traumatic brain injury: a living systematic review and meta-analysis. J Neurotrauma. 2021;38(8):1124-1136.
doi pubmed - Perrin PB, Krch D, Sutter M, Snipes DJ, Arango-Lasprilla JC, Kolakowsky-Hayner SA, Wright J, et al. Racial/ethnic disparities in mental health over the first 2 years after traumatic brain injury: a model systems study. Arch Phys Med Rehabil. 2014;95(12):2288-2295.
doi pubmed - Singh RD, van Dijck J, Maas AIR, Peul WC, van Essen TA. Challenges encountered in surgical traumatic brain injury research: a need for methodological improvement of future studies. World Neurosurg. 2022;161:410-417.
doi pubmed - Ghaith HS, Nawar AA, Gabra MD, Abdelrahman ME, Nafady MH, Bahbah EI, Ebada MA, et al. A literature review of traumatic brain injury biomarkers. Mol Neurobiol. 2022;59(7):4141-4158.
doi pubmed - Barnes DE, Kaup A, Kirby KA, Byers AL, Diaz-Arrastia R, Yaffe K. Traumatic brain injury and risk of dementia in older veterans. Neurology. 2014;83(4):312-319.
doi pubmed - Haarbauer-Krupa J, Pugh MJ, Prager EM, Harmon N, Wolfe J, Yaffe K. Epidemiology of Chronic Effects of Traumatic Brain Injury. J Neurotrauma. 2021;38(23):3235-3247.
doi pubmed - Ponsford JL, Downing MG, Olver J, Ponsford M, Acher R, Carty M, Spitz G. Longitudinal follow-up of patients with traumatic brain injury: outcome at two, five, and ten years post-injury. J Neurotrauma. 2014;31(1):64-77.
doi pubmed - Hicks AJ, Carrington H, Bura L, Yang A, Pesce R, Yew B, Dams-O'Connor K. Blood-based protein biomarkers in the chronic phase of traumatic brain injury: a systematic review. J Neurotrauma. 2025;42(9-10):759-797.
doi pubmed - Graham NSN, Zimmerman KA, Moro F, Heslegrave A, Maillard SA, Bernini A, Miroz JP, et al. Axonal marker neurofilament light predicts long-term outcomes and progressive neurodegeneration after traumatic brain injury. Sci Transl Med. 2021;13(613):eabg9922.
doi pubmed - Maiden MJ, Cameron PA, Rosenfeld JV, Cooper DJ, McLellan S, Gabbe BJ. Long-term outcomes after severe traumatic brain injury in older adults. A registry-based cohort study. Am J Respir Crit Care Med. 2020;201(2):167-177.
doi pubmed - Hawley L, Hammond FM, Cogan AM, Juengst S, Mumbower R, Pappadis MR, Waldman W, et al. Ethical Considerations in Chronic Brain Injury. J Head Trauma Rehabil. 2019;34(6):433-436.
doi pubmed - Orenuga S, Jordache P, Mirzai D, Monteros T, Gonzalez E, Madkoor A, Hirani R, et al. Traumatic brain injury and artificial intelligence: shaping the future of neurorehabilitation-a review. Life (Basel). 2025;15(3):424.
doi pubmed - Beard K, Pennington AM, Gauff AK, Mitchell K, Smith J, Marion DW. Potential applications and ethical considerations for artificial intelligence in traumatic brain injury management. Biomedicines. 2024;12(11):2459.
doi pubmed - van Dijck JTJM, Dijkman MD, Ophuis RH, et al. In-hospital ethics and consent challenges in traumatic brain injury research: a qualitative study. J Neurotrauma. 2020;37(20):2169-2176.
doi - Kompanje EJ, Maas AI, Hilhorst MT, Slieker FJ, Teasdale GM. Ethical considerations on consent procedures for emergency research in severe and moderate traumatic brain injury. Acta Neurochir (Wien). 2005;147(6):633-639; discussion 639-640.
doi pubmed - Stanley RM, Johnson MD, Vance C, Bajaj L, Babcock L, Atabaki S, Thomas D, et al. Challenges enrolling children into traumatic brain injury trials: an observational study. Acad Emerg Med. 2017;24(1):31-39.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Neurology Research is published by Elmer Press Inc.