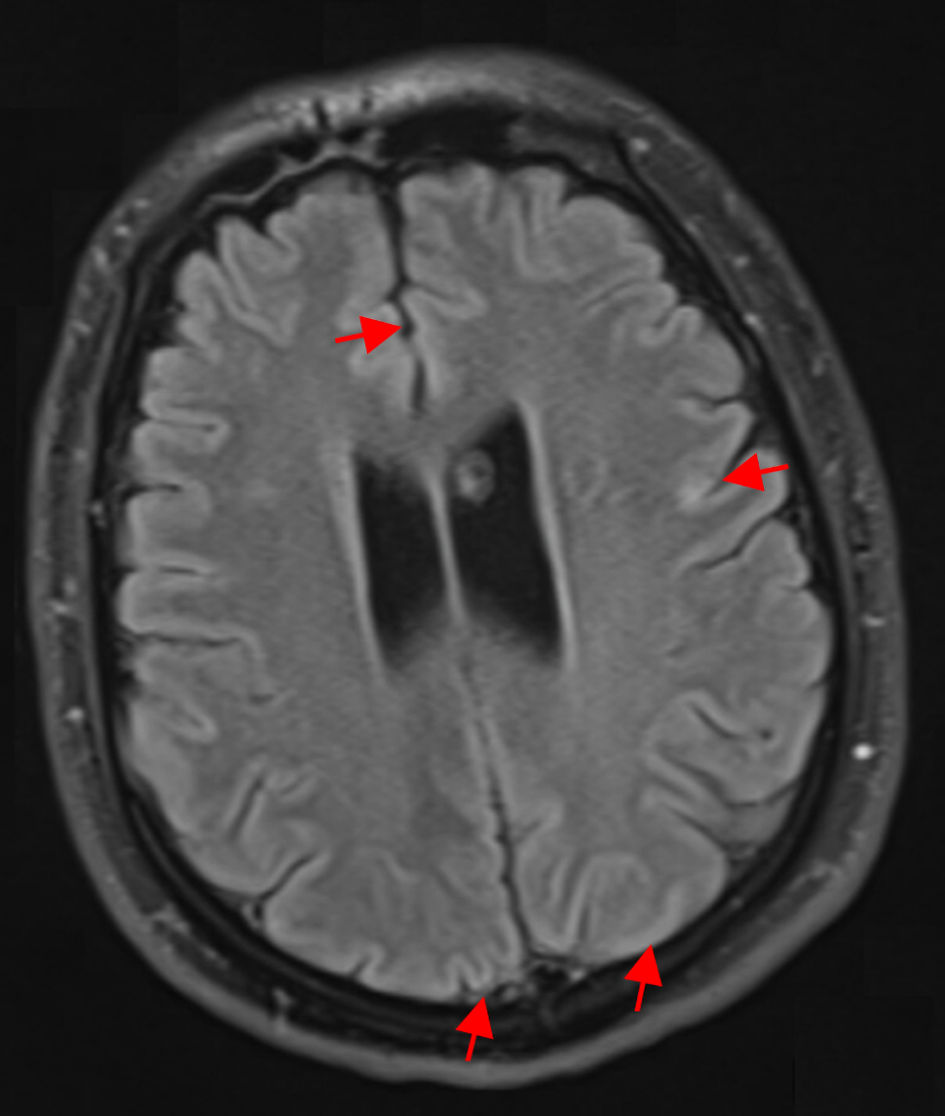
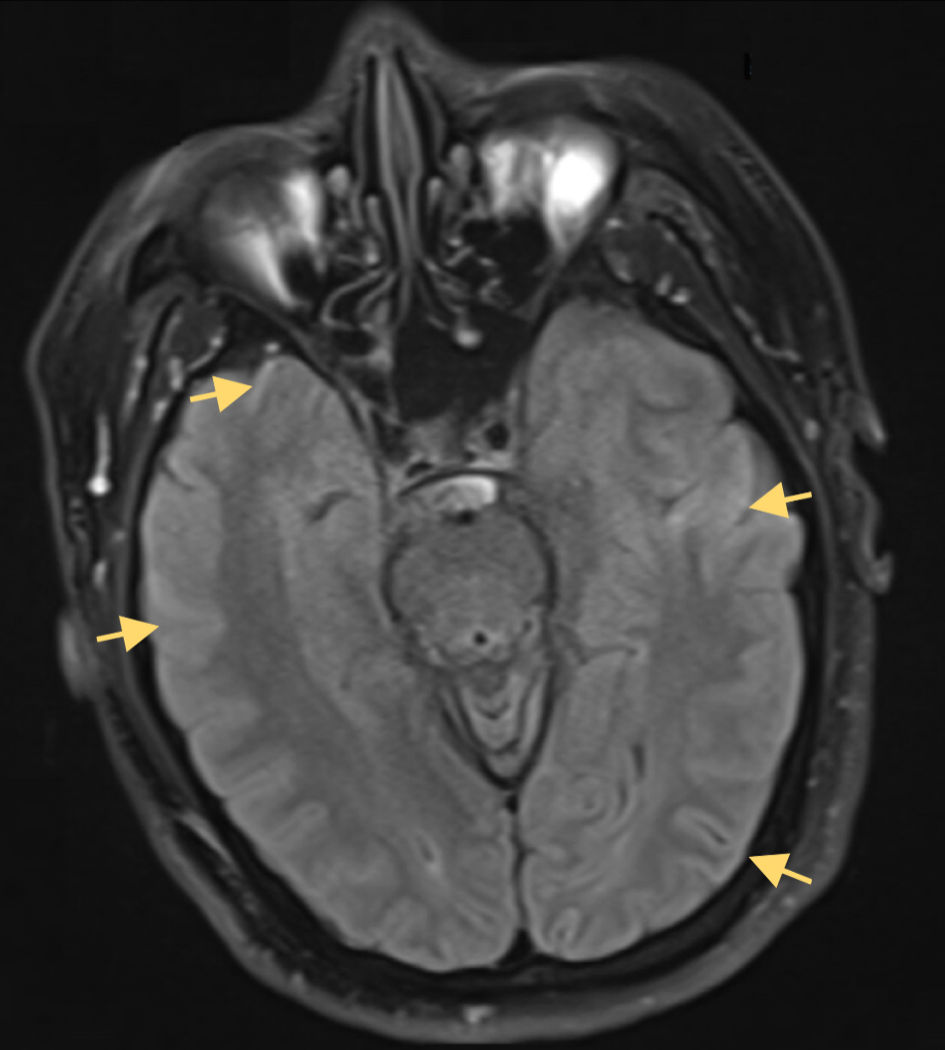
↓ Figure 1. Axial FLAIR MRI without contrast at
the level of the temporal lobes, demonstrating absence of the expected mesial temporal hyperintensities
typically seen in HSV-1 encephalitis. There is curvilinear diffusion hyperintensity in the frontal and
parietal cerebral cortex (red arrows). Both hippocampi, amygdalae, and insular cortices maintain normal
signal intensity and grey-white differentiation. This lack of medial temporal FLAIR hyperintensity is
atypical for HSV-1 encephalitis, which classically presents with unilateral or bilateral temporal lobe
FLAIR hyperintensities and edema. FLAIR: fluid-attenuated inversion recovery; MRI: magnetic resonance
imaging; HSV-1: herpes simplex virus type 1.