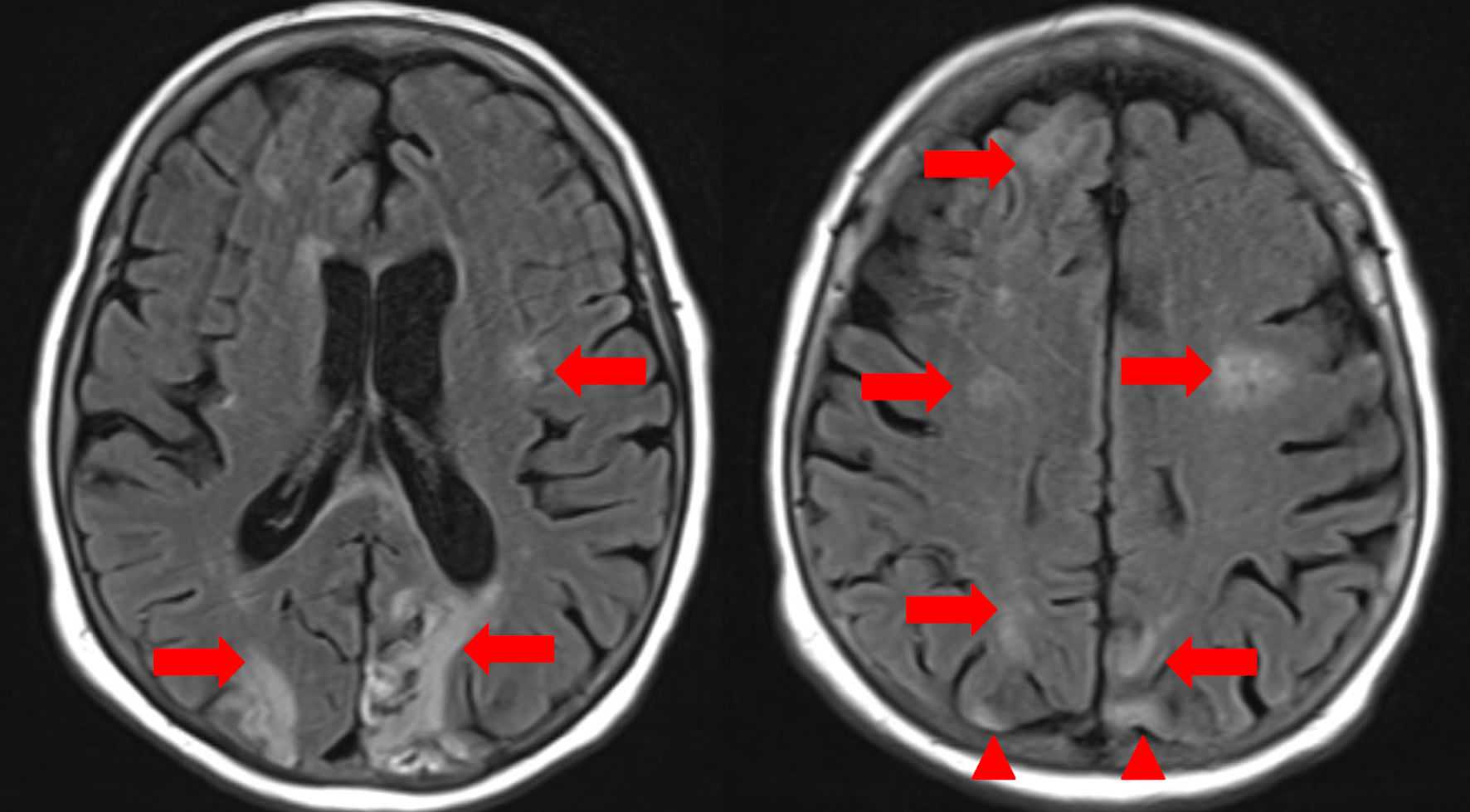
↓ Figure 1. Magnetic resonance imaging (MRI) of
the brain, axial T2-weighted fluid-attenuated inversion recovery (FLAIR) sequences. Red arrows indicate
areas of persistent hyperintensity consistent with evolving acute ischemic infarcts in the bilateral
cerebral hemispheres, notably involving the frontal, parietal, and periventricular white matter regions.
Additional foci in the right frontal and parietal lobes suggest new acute infarcts. Confluent
periventricular hyperintensities are present, compatible with moderate chronic microvascular ischemic
disease. Red arrowheads highlight areas of subacute-to-chronic ischemic injury/encephalomalacia,
demonstrated by parenchymal volume loss and gliotic signal in the bilateral occipital lobes and right
parietal lobe. Multiple small chronic lacunar infarcts are also seen in the corona radiata and centrum
semiovale.
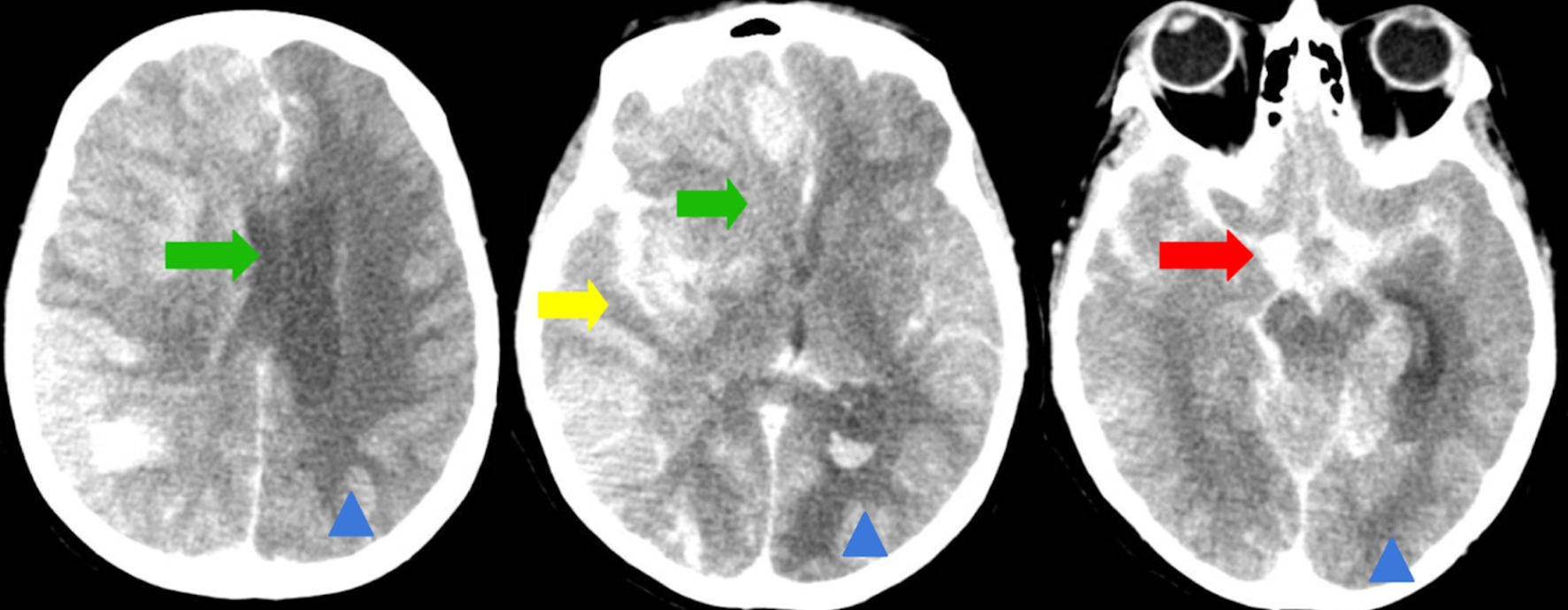
↓ Figure 2. Computed tomography (CT) of the brain
(axial non-contrast). Green arrows indicate a worsening leftward midline shift, now measuring
approximately 12 mm (previously 7 - 8 mm), due to significant hemispheric mass effect. Yellow arrow
highlights hypodensity and swelling in the brainstem and cerebellum, consistent with acute cerebral
edema. Red arrow denotes acute subarachnoid hemorrhage within the basal cisterns and right-sided
cerebral sulci. Chronic ischemic changes, characterized by volume loss and gliosis in the right
occipital lobe and left cerebral hemisphere, would be marked with blue arrowheads for distinction from
acute pathology.
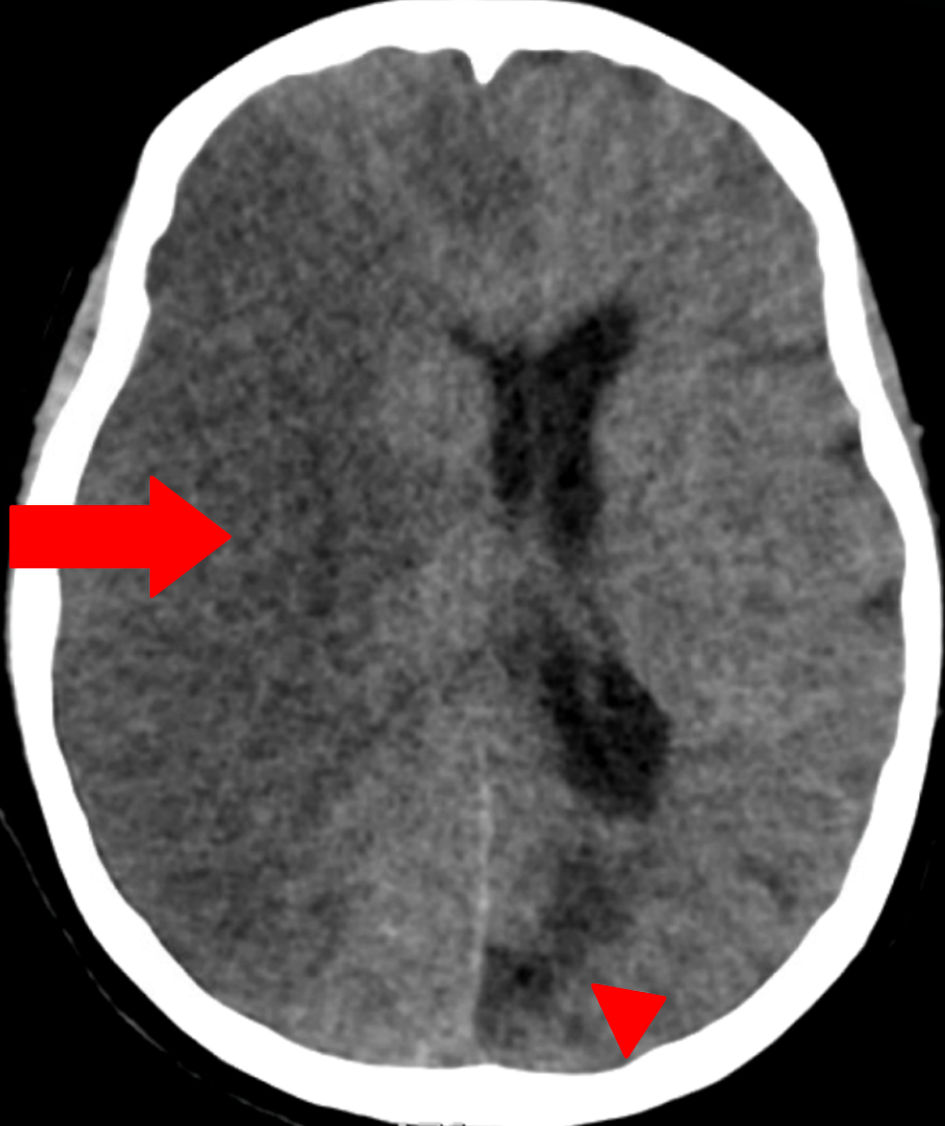
↓ Figure 3. Dual-energy computed tomography
(DECT) of the head (axial view). Red arrow indicates a large area of hypodensity involving the right
cerebral hemisphere, associated with pronounced mass effect and midline shift, consistent with an
extensive acute-to-subacute ischemic infarct. No subarachnoid hemorrhage is seen. Red arrowhead marks an
area of chronic ischemic injury/encephalomalacia in the left occipital region, characterized by
parenchymal volume loss and gliosis. The use of arrowheads differentiates chronic lesions from
acute/subacute pathology.