| Journal of Neurology Research, ISSN 1923-2845 print, 1923-2853 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Neurol Res and Elmer Press Inc |
| Journal website https://jnr.elmerpub.com |
Review
Volume 16, Number 1, March 2026, pages 1-8

Pediatric Facial Nerve Palsy: A Narrative Review of Etiology, Diagnosis, and Management
Adamantios Katerelosa, c, Kalliopi Konstantinopouloub
aDepartment of Neurology, “Karamandaneio” Children’s Hospital, Patras, Greece
bDepartment of Pediatrics, “Karamandaneio” Children’s Hospital, Patras, Greece
cCorresponding Author: Adamantios Katerelos, Department of Neurology, Karamandaneio Children’s Hospital, Patras, Greece
Manuscript submitted October 11, 2025, accepted January 23, 2026, published online March 13, 2026
Short title: Pediatric Facial Nerve Palsy
doi: https://doi.org/10.14740/jnr1057
| Abstract | ▴Top |
Facial nerve palsy (FNP) in children is an uncommon but clinically relevant neurological condition with a broad and age-dependent etiological spectrum. In contrast to adults, pediatric patients present distinct diagnostic challenges related to limited cooperation, subtle clinical signs, and differences in underlying causes, particularly in neonates and young children. These factors may complicate early assessment, severity grading, and management decisions. This narrative review summarizes current evidence on pediatric FNP, focusing on age-related diagnostic considerations, etiological evaluation, severity grading, and evidence-based management. Bell’s palsy represents the most frequent cause of FNP in older children and is generally associated with a favorable prognosis. Accurate differentiation between partial and complete facial palsy at presentation is essential, as severity is a key prognostic factor and guides follow-up intensity and diagnostic workup. Routine neuroimaging and extensive investigations are not required in children with typical, isolated facial palsy and partial weakness, while targeted diagnostic evaluation should be reserved for atypical presentations, complete paralysis, associated neurological deficits, or lack of early clinical improvement. Corticosteroid therapy may be considered in moderate to severe cases of Bell’s palsy when initiated early, whereas routine antiviral treatment and surgical interventions are not supported by current pediatric evidence. Most children experience spontaneous recovery, and rehabilitation strategies should be individualized. An age-specific, severity-based, and etiology-driven approach is essential for optimal management of pediatric FNP, helping to avoid unnecessary investigations and overtreatment while ensuring appropriate follow-up and care.
Keywords: Facial nerve palsy; Children Bell’s palsy; Prognosis; Pediatric neurology
| Introduction | ▴Top |
Facial nerve palsy (FNP) in children represents a distinct clinical entity that differs substantially from adult facial paralysis in terms of etiology, diagnostic challenges, management strategies, and prognosis. Although idiopathic peripheral facial palsy (Bell’s palsy) remains the most common cause, pediatric FNP encompasses a broad spectrum of congenital, infectious, inflammatory, traumatic, and systemic conditions that require careful evaluation [1–3].
One of the principal challenges in pediatric FNP is diagnostic uncertainty. Unlike adults, children—particularly neonates and infants—may be unable to cooperate during clinical examination, making the identification of facial asymmetry, the affected side, and the severity of paralysis difficult [4, 5]. Moreover, the clinical signs typically used in adults, such as voluntary facial expressions or eye closure asymmetry, may be subtle or unreliable in younger age groups. As a result, misclassification of severity and delayed diagnosis are not uncommon in pediatric practice [2, 6].
A further critical issue is the differentiation between partial (incomplete) and complete (total) facial palsy, which has major implications for prognosis, monitoring, and management. Partial facial palsy in children is generally associated with an excellent prognosis and often resolves spontaneously, whereas complete paralysis warrants closer follow-up and, in selected cases, further diagnostic investigations [3, 7]. The early and systematic use of validated grading systems, such as the House–Brackmann scale, is therefore essential for clinical decision-making and longitudinal assessment [7, 8].
In addition, pediatric FNP should be approached in an age-specific manner. Neonatal and early infantile facial palsy is frequently related to birth trauma or congenital syndromes and differs markedly from facial palsy in older children and adolescents, whose etiological profile increasingly resembles that of adults [4, 9]. Failure to recognize these age-related differences may lead to inappropriate investigations or overtreatment.
The aim of this narrative review is to provide a clinically oriented synthesis of current evidence on pediatric FNP, with particular emphasis on diagnostic challenges, age-based evaluation, severity grading, and evidence-supported management strategies. By focusing on practical aspects of daily clinical care, this review seeks to clarify common areas of uncertainty and highlight gaps requiring further research.
| Definition and Classification of Pediatric FNP | ▴Top |
FNP is defined as weakness or paralysis of the muscles innervated by the seventh cranial nerve (VII CN), resulting in impaired facial movement and asymmetry. In pediatric patients, FNP may be classified according to anatomical localization, severity, and temporal course, each of which has diagnostic and prognostic relevance.
Peripheral versus central FNP
From a clinical standpoint, pediatric FNP is most usefully categorized as peripheral or central. Peripheral FNP results from lesions affecting the facial nerve nucleus or its extracranial course and is characterized by weakness of both the upper and lower facial muscles on the affected side, including the forehead [10, 11]. In contrast, central facial palsy, typically due to supranuclear lesions, spares the forehead because of bilateral cortical innervation and is usually associated with additional neurological deficits [12, 13]. While central causes are rare in children, they have to be considered in cases with atypical presentation or associated neurological signs [14].
Partial versus complete facial palsy
Severity-based classification is of paramount importance in pediatric FNP. Partial (incomplete) facial palsy refers to preserved but weakened facial movements, whereas complete (total) facial palsy denotes the absence of voluntary movement in all facial regions on the affected side. This distinction is not merely descriptive but directly influences prognosis and management. Partial palsy in children is associated with high rates of spontaneous recovery, often exceeding 90%, whereas complete palsy carries a higher risk of delayed recovery and residual deficits [3, 7].
The House–Brackmann grading system remains the most widely used tool for assessing facial nerve function in both adults and children (Table 1). Despite certain limitations in very young or uncooperative patients, early application of this grading system allows objective documentation of severity, guides follow-up intensity, and supports treatment decisions, particularly in cases of complete paralysis [7, 8].
 Click to view | Table 1. The House-Brackmann Grading System |
| Age-Based Diagnostic Approach to Pediatric FNP | ▴Top |
An age-specific diagnostic framework is essential for the accurate evaluation of pediatric FNP, as the underlying causes and clinical features vary significantly across different developmental stages.
Neonates and newborns
FNP presenting at birth or in the neonatal period is most commonly related to birth trauma, particularly following prolonged labor, instrumental delivery, or malpositioning during delivery [4, 15]. Postpartum facial palsy typically manifests as unilateral weakness noted during crying or feeding and is often transient, with spontaneous recovery occurring within weeks to months [15]. Congenital causes, including facial nerve agenesis or syndromic conditions such as Moebius syndrome (MBS) should be suspected in cases of bilateral palsy, associated craniofacial anomalies, or absence of recovery [9, 16].
Clinical assessment in neonates is particularly challenging, as facial asymmetry may be subtle at rest and more apparent only during crying. Careful observation during feeding and crying, combined with a detailed perinatal history, is therefore essential [4].
Infants and young children
In infants and young children, infectious and inflammatory etiologies become more prominent. Acute otitis media, viral infections, and Lyme disease are well-recognized causes of pediatric FNP in this age group [2, 17]. Unlike adults, classical signs such as incomplete eye closure or the Charles Bell phenomenon may be difficult to assess reliably, emphasizing the importance of repeated examinations and parental observations [5].
Older children and adolescents
In older children and adolescents, the etiological spectrum of FNP increasingly resembles that seen in adults, with Bell’s palsy accounting for the majority of cases [1, 3]. Functional or psychogenic facial weakness should also be considered in adolescents presenting with atypical features or inconsistent examination findings [18]. At this age, standardized grading systems and patient-reported symptoms can be applied more reliably to guide management and follow-up.
| Etiology of Pediatric FNP | ▴Top |
The etiology of pediatric FNP is heterogeneous and strongly influenced by age, clinical presentation, and severity of paralysis. Although idiopathic peripheral facial palsy (Bell’s palsy) remains the most frequent diagnosis, accounting for the majority of cases in older children, a wide range of infectious, congenital, inflammatory, traumatic, and systemic causes have to be considered, particularly in atypical or severe presentations [1–3].
Bell’s palsy typically presents as acute, unilateral peripheral FNP without systemic illness and carries a favorable prognosis in children [1, 7]. Viral triggers, including herpes simplex virus (HSV) and varicella–zoster virus (VZV), have been implicated, although definitive causality remains unproven in pediatric populations [19, 20]. Infectious causes such as Lyme disease and Epstein–Barr virus (EBV) infection represent important differential diagnoses, especially in endemic regions or in cases with systemic symptoms, bilateral involvement, or incomplete recovery [17, 21, 22].
Inflammatory and autoimmune conditions, including Guillain–Barré syndrome (GBS), should be suspected when facial palsy is bilateral or associated with limb weakness, areflexia, or cranial polyneuropathy [23–25]. In such cases, FNP is rarely isolated and often reflects broader neurological involvement.
Congenital and syndromic causes, such as MBS and Melkersson–Rosenthal syndrome, are rare but uniquely pediatric entities. These conditions typically present early in life, often with bilateral facial weakness and associated craniofacial or neurological abnormalities, and require specialized diagnostic and rehabilitative approaches [9, 16].
Traumatic FNP may occur following temporal bone fractures, birth-related injury, or iatrogenic damage during otologic or parotid surgery. The onset may be immediate or delayed, and prognosis depends on the extent of nerve injury and the timing of intervention [8, 26, 27]. Neoplastic causes of pediatric FNP are rare and usually characterized by progressive or recurrent symptoms rather than acute onset, warranting targeted imaging when suspected [14, 28].
The most common and clinically relevant etiologies, stratified by age, presentation, and level of evidence, are summarized in Table 2.
Click to view | Table 2. Major etiologies of pediatric facial nerve palsy according to age, clinical presentation, and evidence level |
| Clinical Assessment and Diagnostic Workup | ▴Top |
Accurate clinical assessment is fundamental in the evaluation of pediatric FNP and represents the cornerstone of diagnostic decision-making. A structured neurological examination allows early identification of disease severity, anatomical localization, and potential red flags suggestive of secondary or serious underlying pathology. Given the heterogeneous etiology of pediatric FNP, careful clinical stratification is essential to guide follow-up intensity and the need for further investigations [3, 7].
Clinical Assessment and Severity Grading
A thorough neurological examination remains the cornerstone of assessment in pediatric FNP. Early differentiation between partial and complete facial paralysis is essential, as it directly influences prognosis, follow-up intensity, and subsequent management decisions [3, 7]. Clinical evaluation should focus on facial symmetry at rest, voluntary facial movements, degree of eye closure, forehead involvement, and the presence of associated neurological signs.
Objective severity grading at presentation and during follow-up is strongly recommended. The House–Brackmann grading system should be applied to document disease progression or recovery, although assessment may be challenging in neonates and very young children [7, 8]. Despite these limitations, the House–Brackmann scale remains the most widely used clinical tool for severity classification and provides a practical framework for prognostic stratification, follow-up planning, and treatment considerations in pediatric practice (Table 1).
In cases of complete facial paralysis, closer clinical surveillance is warranted. Daily or frequent monitoring by clinicians, caregivers, or trained nursing staff may facilitate early recognition of recovery, exposure-related ocular complications, or evolving neurological signs requiring reassessment [3, 8].
Accurate clinical assessment is fundamental in the evaluation of pediatric FNP and represents the cornerstone of diagnostic decision-making. A structured neurological examination allows early identification of disease severity, anatomical localization, and potential red flags that may indicate secondary or serious underlying pathology. Given the wide etiological spectrum of pediatric FNP, careful clinical stratification is essential to guide follow-up intensity and the need for further investigations.
Anatomical localization: central versus peripheral facial palsy
Clinical differentiation between central (upper motor neuron) and peripheral (lower motor neuron) facial palsy is a critical early step in the diagnostic process, guiding subsequent imaging and etiological investigation. Central facial palsy typically spares the forehead and is often associated with additional neurological deficits, whereas peripheral facial palsy involves the entire hemiface and reflects pathology affecting the facial nerve itself [14, 28].
A schematic overview of the typical patterns of facial weakness is provided in Figure 1, serving as a practical aid for initial neurological localization during clinical assessment.
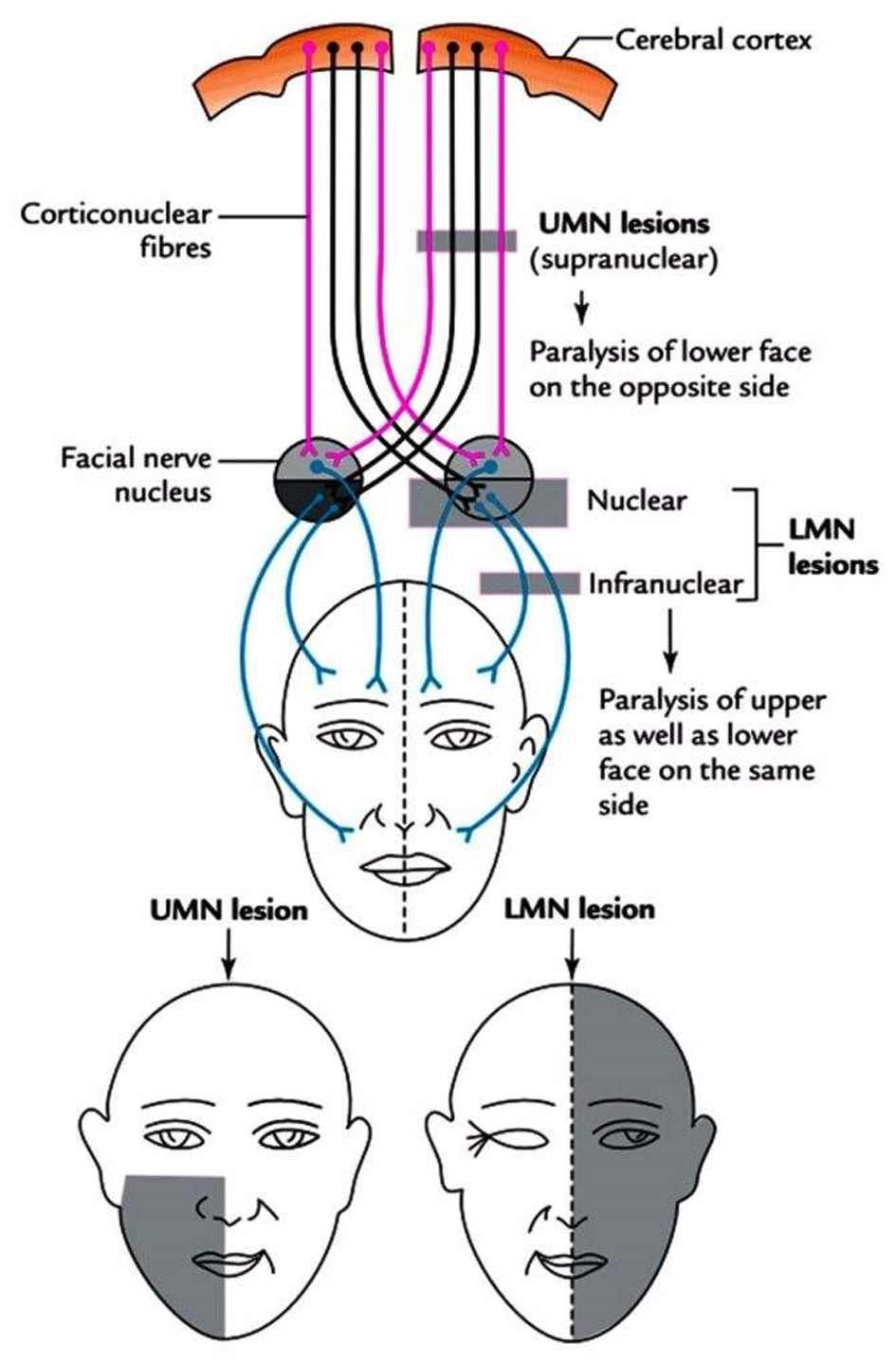 Click for large image | Figure 1. Schematic representation of upper motor neuron (central) and lower motor neuron (peripheral) facial palsy patterns. The figure illustrates basic anatomical and clinical differences relevant to initial neurological assessment (Photo by Dr. Rahul Bagla ENT Textbook, used with permission). |
Imaging and additional investigations
Neuroimaging is not routinely required in children presenting with typical, uncomplicated peripheral facial palsy and favorable early clinical evolution. However, imaging should be considered in the presence of atypical features, including progressive or recurrent symptoms, bilateral facial palsy, lack of clinical improvement over time, or associated neurological deficits [3, 14, 28].
Magnetic resonance imaging (MRI) is the preferred modality when central nervous system (CNS) pathology, inflammatory conditions, neoplastic processes, or structural lesions are suspected. Computed tomography (CT) may be indicated in cases of traumatic facial palsy, particularly when temporal bone fractures are suspected [8, 26]. Additional laboratory testing or neurophysiological studies should be guided by clinical suspicion and the underlying etiological context rather than performed routinely [3, 7].
| Management of Pediatric FNP | ▴Top |
Management of pediatric FNP should be individualized according to etiology, patient age, and severity of paralysis, with particular emphasis on the distinction between partial and complete palsy. Given the generally favorable prognosis observed in most pediatric cases, overtreatment should be avoided, especially in children with partial paralysis and early clinical improvement. Management decisions should therefore be etiology-driven and severity-based rather than protocol-oriented. An indication-based overview of recommended and non-recommended management strategies across the most common pediatric scenarios is provided in Table 3.
Click to view | Table 3. Management of Pediatric Facial Nerve Palsy: Indication-Based Approach |
Bell’s palsy in children
Bell’s palsy represents the most common cause of pediatric FNP and remains one of the most debated entities in terms of optimal management. Although corticosteroids are widely prescribed in clinical practice, high-quality evidence in pediatric populations remains limited compared with adult studies. Available data suggest that early administration of corticosteroids, ideally within 72 h of symptom onset, may accelerate recovery and improve facial symmetry, particularly in children presenting with moderate to severe facial palsy [7, 29]. Treatment courses are typically short and weight-adjusted, with careful consideration of potential adverse effects.
As outlined in Table 3, routine pharmacological treatment is not required in children with partial facial palsy and early clinical improvement, whereas corticosteroid therapy may be considered in moderate to severe cases when initiated within the first 72 h. This severity-based approach aims to balance potential therapeutic benefit against the risk of unnecessary medication exposure.
The routine use of antiviral therapy in pediatric Bell’s palsy is not supported by current evidence. Antivirals may be considered in selected cases with suspected viral etiology; however, available data do not demonstrate a clear benefit when used as monotherapy, and their adjunctive role remains uncertain [30, 31].
Surgical intervention has no role in the routine management of pediatric Bell’s palsy. Facial nerve decompression or reconstructive procedures should be reserved for exceptional cases with documented nerve compression, traumatic injury, or neoplastic involvement, and only after a prolonged absence of spontaneous recovery [26, 32].
Management of other etiologies
Management of secondary causes of pediatric FNP is directed primarily toward treatment of the underlying condition. In Lyme disease–associated facial palsy, prompt initiation of appropriate antibiotic therapy is essential and is associated with excellent neurological outcomes [17, 22]. In GBS, facial nerve involvement is rarely isolated, and treatment with intravenous immunoglobulin (IVIG) or plasmapheresis is guided by overall neurological severity rather than facial palsy alone [23, 25].
Traumatic FNP may require early surgical consultation when radiological findings or clinical progression suggest nerve disruption or severe axonal injury. In contrast, incomplete traumatic palsy with evidence of early recovery is generally managed conservatively [8]. Across all secondary etiologies, multidisciplinary evaluation and etiology-specific management remain central to optimizing outcomes.
| Rehabilitation and Supportive Care in Children | ▴Top |
Rehabilitation strategies in pediatric FNP differ from those in adults. Most children experience spontaneous recovery, and routine physiotherapy is not universally required. Facial exercises and targeted rehabilitation may be beneficial in cases with delayed recovery, residual weakness, or following surgical nerve repair [26, 33].
The use of electrical stimulation in children remains controversial due to limited evidence, potential discomfort, and concerns regarding synkinetic or spastic sequelae; therefore, it is not routinely recommended [34]. Similarly, low-level laser therapy should be considered experimental, with insufficient evidence to support routine clinical use in pediatric populations [35].
Psychological support should not be overlooked. Facial palsy can affect not only the child but also parents and caregivers, particularly when recovery is prolonged or asymmetry persists [36, 37]. Clear communication regarding prognosis and expected recovery is an essential component of care.
| Prognosis and Follow-Up | ▴Top |
The prognosis of pediatric FNP is generally favorable and is primarily determined by the etiology, the severity of paralysis at presentation, and the timing of clinical improvement. Among children with Bell’s palsy, complete functional recovery occurs in approximately 80–90% of cases, often within the first 3–4 months following onset [3, 29, 38].
Severity grading at presentation is a key prognostic factor. Children presenting with partial facial palsy (House–Brackmann grades II–III) typically demonstrate rapid and complete recovery, frequently without the need for pharmacological or rehabilitative intervention [3, 7]. In contrast, complete facial palsy (grades IV–VI) is associated with slower recovery and a higher likelihood of residual weakness or synkinesis, underscoring the importance of close clinical follow-up in this subgroup [39, 40].
Early clinical improvement, usually within the first 2–3 weeks, is a favorable prognostic indicator, whereas absence of recovery signs beyond this period should prompt reconsideration of the diagnosis and further evaluation [41, 42]. Etiology-specific prognosis must also be considered. Facial palsy associated with Lyme disease or other infections typically resolves fully with appropriate treatment, while recovery in GBS depends on the extent of overall neurological involvement rather than facial nerve dysfunction alone [22, 25].
Long-term complications, including synkinesis, facial asymmetry, and incomplete recovery, are uncommon in children but may occur, particularly after severe or prolonged paralysis [37, 43]. Regular follow-up using standardized grading systems is therefore recommended until stable recovery is achieved.
| Conclusion: What Do We Learn for Clinical Practice? | ▴Top |
Pediatric FNP is a heterogeneous condition that requires an approach distinct from that used in adults. Accurate diagnosis relies on careful clinical assessment, early severity grading, and age-specific evaluation rather than extensive routine investigations.
Several key clinical principles emerge from current evidence. First, differentiation between partial and complete facial palsy at presentation is crucial, as it directly influences prognosis, follow-up intensity, and management decisions. Partial facial palsy in children is associated with excellent spontaneous recovery, whereas complete paralysis warrants closer monitoring and, in selected cases, further diagnostic evaluation.
Second, management should be etiology-driven and conservative whenever possible. Bell’s palsy, the most common cause of pediatric FNP, generally has a favorable outcome. Corticosteroids may be considered in moderate to severe cases when initiated early, while routine use of antivirals or surgical interventions is not supported by current pediatric evidence.
Third, rehabilitation strategies in children differ from those in adults. Routine physiotherapy or electrical stimulation is rarely required and should be reserved for selected cases with delayed recovery or post-surgical nerve repair. Clear communication with families regarding expected recovery and prognosis is essential to avoid unnecessary anxiety and overtreatment.
Finally, the use of standardized grading systems and structured follow-up allows objective assessment of recovery and early identification of atypical courses. Future research should focus on prospective, pediatric-specific studies to refine diagnostic pathways and establish evidence-based management guidelines tailored to children.
Acknowledgments
The authors have no acknowledgments to declare.
Financial Disclosure
The authors declare no financial support.
Conflict of Interest
The authors declare no conflict of interest.
Author Contributions
AK and KK conceptualized and designed the study. Literature screening, data extraction, and critical appraisal were performed by AK and KK. Data interpretation and analysis were cross-checked by AK. The manuscript was drafted by KK and critically revised by AK. Both authors participated in the interpretation of the findings, contributed intellectually throughout the study, and approved the final version of the manuscript.
Data Availability
No new data were generated or analyzed in this study. All data supporting the findings of this review are derived from published literature and are available within the article.
Abbreviations
CEBM: Centre for Evidence-Based Medicine; CNS: central nervous system; CT: computed tomography; EBV: Epstein–Barr virus; FNP: facial nerve palsy; GBS: Guillain–Barré syndrome; HSV: herpes simplex virus; IV: intravenous; IVIG: intravenous immunoglobulin; LMN: lower motor neuron; MBS: Moebius syndrome; MRI: magnetic resonance imaging; UMN: upper motor neuron; VII CN: seventh cranial nerve; VZV: varicella–zoster virus
| References | ▴Top |
- Ozkale Y, Erol I, Saygi S, Yilmaz I. Overview of pediatric peripheral facial nerve paralysis: analysis of 40 patients. J Child Neurol. 2015;30(2):193-199.
doi pubmed - Castellazzi ML, Torretta S, Pietro GMD, Ciabatta A, Capaccio P, Caschera L, Marchisio P. Acute otitis media-related facial nerve palsy in a child: a case report and a literary review. Ital J Pediatr. 2023;49(1):8.
doi pubmed - Psillas G, Antoniades E, Ieridou F, Constantinidis J. Facial nerve palsy in children: a retrospective study of 124 cases. J Paediatr Child Health. 2019;55(3):299-304.
doi pubmed - Baelen H, Esschendal AM, De Brucker Y, Foulon I, Topsakal V, Gordts F. Congenital facial nerve palsy: Single center study. Front Pediatr. 2023;11:1077238.
doi pubmed - Yilmaz U, Cubukcu D, Yilmaz TS, Akinci G, Ozcan M, Guzel O. Peripheral facial palsy in children. J Child Neurol. 2014;29(11):1473-1478.
doi pubmed - Swain S, Behera I, Sahu M. Bell’s palsy among infants - our experiences in a tertiary care hospital of eastern India. Asian Journal of Pharmaceutical and Clinical Research. 2017;10(9):85.
- Pitaro J, Waissbluth S, Daniel SJ. Do children with Bell's palsy benefit from steroid treatment? A systematic review. Int J Pediatr Otorhinolaryngol. 2012;76(7):921-926.
doi pubmed - Kanona H, Anderson C, Lambert A, Al-Abdulwahed R, O'Byrne L, Vakharia N, Motter D, et al. A large case series of temporal bone fractures at a UK major trauma centre with an evidence-based management protocol. J Laryngol Otol. 2020;134(3):205-212.
doi pubmed - Ali MH, Jamal S, Rashid MA, Javaid U, Butt NH. Moebius syndrome with hypoglossal palsy, syndactyly, brachydactyly, and anisometropic amblyopia. Cureus. 2018;10(3):e2334.
doi pubmed - Terada K, Niizuma T, Kosaka Y, Inoue M, Ogita S, Kataoka N. Bilateral facial nerve palsy associated with Epstein-Barr virus infection with a review of the literature. Scand J Infect Dis. 2004;36(1):75-77.
doi pubmed - Ting CH, Wang CW, Lee JT, Peng GS, Yang FC. Bilateral facial nerve palsy as the sole initial symptom of syphilis: a case report. CJEM. 2015;17(5):576-581.
doi pubmed - Burson K, Mastenbrook J, Van Dommelen K, Shah M, Bauler LD. A focal pontine infarct presenting as unilateral facial nerve paralysis. Cureus. 2020;12(9):e10646.
doi pubmed - Phipps K, Joea R, Strube S, Carrillo-Nunez I. Pontine infarct camouflaged as Bell’s Palsy. Journal of Neurology Research. 2019;9(1-2):14-17.
- Ismail MT, Rahman RA, Idris NS. When paediatric facial nerve paralysis is not a Bell's palsy: A case of cerebellopontine angle tumour. J Taibah Univ Med Sci. 2022;17(1):141-145.
doi pubmed - Pandita A, Mishra N, Gupta G, Shukla A. Neonatal facial palsy, a case series: is CPAP the culprit? BMJ Case Rep. 2018.
doi pubmed - Okudo J, Oluyide Y. Melkersson-rosenthal syndrome with orofacial swelling and recurrent lower motor neuron facial nerve palsy: a case report and review of the literature. Case Rep Otolaryngol. 2015;2015:214946.
doi pubmed - Tveitnes D, Oymar K, Natas O. Acute facial nerve palsy in children: how often is it lyme borreliosis? Scand J Infect Dis. 2007;39(5):425-431.
doi pubmed - Klau J, Abou Jamra R, Radtke M, Oppermann H, Lemke JR, Beblo S, Popp B. Exome first approach to reduce diagnostic costs and time - retrospective analysis of 111 individuals with rare neurodevelopmental disorders. Eur J Hum Genet. 2022;30(1):117-125.
doi pubmed - Folayan MO, Arobieke RI, Eziyi E, Oyetola EO, Elusiyan J. Facial nerve palsy: analysis of cases reported in children in a suburban hospital in Nigeria. Niger J Clin Pract. 2014;17(1):23-27.
doi pubmed - Ogita S, Terada K, Niizuma T, Kosaka Y, Kataoka N. Characteristics of facial nerve palsy during childhood in Japan: frequency of varicella-zoster virus association. Pediatr Int. 2006;48(3):245-249.
doi pubmed - Broekhuijsen-van Henten DM, Braun KP, Wolfs TF. Clinical presentation of childhood neuroborreliosis; neurological examination may be normal. Arch Dis Child. 2010;95(11):910-914.
doi pubmed - Marques A, Okpali G, Liepshutz K, Ortega-Villa AM. Characteristics and outcome of facial nerve palsy from Lyme neuroborreliosis in the United States. Ann Clin Transl Neurol. 2022;9(1):41-49.
doi pubmed - Bhargava A, Banakar BF, Pujar GS, Khichar S. A study of Guillain-Barre syndrome with reference to cranial neuropathy and its prognostic implication. J Neurosci Rural Pract. 2014;5(Suppl 1):S43-47.
doi pubmed - Narayanan RP, James N, Ramachandran K, Jaramillo MJ. Guillain-Barre Syndrome presenting with bilateral facial nerve paralysis: a case report. Cases J. 2008;1(1):379.
doi pubmed - Sharma K, Tengsupakul S, Sanchez O, Phaltas R, Maertens P. Guillain-Barre syndrome with unilateral peripheral facial and bulbar palsy in a child: A case report. SAGE Open Med Case Rep. 2019;7:2050313X19838750.
doi pubmed - Liu Y, Han J, Zhou X, Gao K, Luan D, Xie F, Wang X, et al. Surgical management of facial paralysis resulting from temporal bone fractures. Acta Otolaryngol. 2014;134(6):656-660.
doi pubmed - Dubey R, Panchal S, Ahmed J, et al. Delayed facial palsy after head injury- a prospective study conducted at a tertiary care centre. Journal of Evolution of Medical and Dental Sciences. 2019;8(50):3785-3789.
- Rastogi N. Intraparotidschwannoma of facial nerve: a case report. Asian Pacific Journal of Health Sciences. 2017;4(1):190-191.
- Shokri T, Saadi R, Schaefer EW, Lighthall JG. Trends in the treatment of Bell's palsy. Facial Plast Surg. 2020;36(5):628-634.
doi pubmed - Manjit Singh P, Abdul Kashaf N, Alias A, Nik Othman N. Incidental finding of facial schwannoma: a case report. Egyptian Journal of Ear, Nose, Throat and Allied Sciences. 2021;22(22):1-3
- Unuvar E, Toprak S, Bayhan GI, Aytac K, Ciftci E, Kara A, et al. Use of acyclovir in pediatric Bell’s palsy: a multicenter retrospective study. Pediatr Infect Dis J. 2014;33(7):710-714.
- Alwan M, Gordan M. Facial nerve baroparesis during airflight: a case report and literature review. J Laryngol Otol. 2021;135(1):88-92.
doi pubmed - Cubukcu D, Yilmaz U, AlkanH, et al. Clinical features of Bell’s palsy in children and outcomes of physical therapy: a retrospective study. International Scholarly Research Notices. 2013;2013:1-6.
- Sommerauer L, Engelmann S, Ruewe M, Anker A, Prantl L, Kehrer A. Effects of electrostimulation therapy in facial nerve palsy. Arch Plast Surg. 2021;48(3):278-281.
doi pubmed - Shoman A, Hassan A, Kassab A. A study on the effect of 850 nm low-level diode laser versus electrical stimulation in facial nerve regeneration for patients with Bell's palsy. ORL J Otorhinolaryngol Relat Spec. 2022;84(5):370-377.
doi pubmed - Greene JJ, Sadjadi R, Jowett N, Hadlock T. Facial palsy, radiographic and other workup negative: FROWN. Neurol Clin Pract. 2021;11(5):e654-e660.
doi pubmed - Faris C, Tessler O, Heiser A, Hadlock T, Jowett N. Evaluation of societal health utility of facial palsy and facial reanimation. JAMA Facial Plast Surg. 2018;20(6):480-487.
doi pubmed - Zhang Q, Zhu C, Liu J. Kinesitherapy for idiopathic facial palsy: a protocol of systematic review and meta-analysis. Medicine (Baltimore). 2020;99(52):e23902.
doi pubmed - Alencar TN, Botelho MM, Carasek N, Bahmad F, Jr. Surgical treatment outcome for familial Melkersson-Rosenthal syndrome. Am J Case Rep. 2023;24:e938670.
doi pubmed - Neamonitou F, Kotrotsiou M, Stavrianos S. Dynamic surgical restoration of mid and lower facial paralysis: a single-greek-centre experience. Cureus. 2024;16(1):e52387.
doi pubmed - Wamkpah NS, Kallogjeri D, Snyder-Warwick AK, Buss JL, Durakovic N. Incidence and Management of Facial Paralysis After Skull Base Trauma, an Administrative Database Study. Otol Neurotol. 2022;43(10):e1180-e1186.
doi pubmed - Fana M, Centofanti B, Kuriakose P. Chemotherapy as treatment for acute myeloid leukemia (AML)-induced facial nerve palsy. Cureus. 2022;14(3):e23710.
doi pubmed - Guntinas-Lichius O, Prengel J, Cohen O, Makitie AA, Vander Poorten V, Ronen O, Shaha A, et al. Pathogenesis, diagnosis and therapy of facial synkinesis: A systematic review and clinical practice recommendations by the international head and neck scientific group. Front Neurol. 2022;13:1019554.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Neurology Research is published by Elmer Press Inc.