| Journal of Neurology Research, ISSN 1923-2845 print, 1923-2853 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Neurol Res and Elmer Press Inc |
| Journal website https://jnr.elmerpub.com |
Case Report
Volume 16, Number 2, June 2026, pages 122-126

Adult-Onset Reversible Splenial Lesion Syndrome: A Case Series and Review of Age-Related Differences
Khaoula Belaidia, b, c ![]() , Safae Zahlanea, b, M’Hamed Riad Amanallaha, b, Oumayna Azzoua, b, Hamza Benzakoura, b, Yasmina Zakariaa, b, Mohamed Chraaa, b, Nissrin Louhaba, b
, Safae Zahlanea, b, M’Hamed Riad Amanallaha, b, Oumayna Azzoua, b, Hamza Benzakoura, b, Yasmina Zakariaa, b, Mohamed Chraaa, b, Nissrin Louhaba, b
aNeurology Department, Mohammed VI University Hospital, Marrakech, Morocco
bMarrakech Medical School, Cadi Ayyad University, Marrakech, Morocco
cCorresponding Author: Khaoula Belaidi, Neurology Department, Mohammed VI University Hospital, Marrakesh, Morocco
Manuscript submitted December 11, 2025, accepted March 11, 2026, published online May 4, 2026
Short title: Adult-Onset RESLES
doi: https://doi.org/10.14740/jnr1085
| Abstract | ▴Top |
Reversible splenial lesion syndrome (RESLES) is a neuroradiological entity described by a reversible lesion in the splenium of the corpus callosum (SCC) of unknown etiology. RESLES is often associated with infectious and metabolic diseases, seizure, and antiepileptic drugs withdrawal. Although clinical presentations are nonspecific, the syndrome is typically identified by its radiological aspects through magnetic resonance imaging (MRI). In this report, we present five cases of adult-onset RESLES (two males and three females) that were admitted in our department at a university hospital in the years between 2021 and 2025, with each case occurring in different clinical settings. We analyze their presentation, clinical course, and outcomes, and compare them with pediatric-onset cases to highlight potential age-related differences. Patients’ ages varied from 29 to 46 years old. Neurological symptoms included: headache 3/5, drowsiness 2/5, slurred speech 2/5, hearing loss 1/5, blurred vision 1/5, dysarthria 1/5, limb ataxia 1/5, postural tremors 1/5, insomnia 1/5, and agitation 1/5. One patient presented with a unique seizure then remained asymptomatic. The clinical settings associated with RESLES included the postpartum, infection, multiple organ failure, extensive cerebral venous thrombosis, and Burkitt lymphoma. Clinical outcomes at follow-up were favorable across all cases. In contrast to pediatric-onset RESLES, where symptoms and precipitating factors appear relatively homogeneous across studies with seizures as the predominant manifestation and infection as the leading cause, adult-onset cases demonstrate greater clinical and etiological heterogeneity. Analysis of our sample suggests that adult-onset RESLES shares the core radiological characteristics of the pediatric form but differs markedly in its common precipitating factors and clinical presentations.
Keywords: Splenium of the corpus callosum; Reversible splenial lesion syndrome; Magnetic resonance imaging
| Introduction | ▴Top |
Reversible splenial lesion syndrome (RESLES) is a rare but well-defined neuroradiological condition characterized by a transient, isolated lesion in the splenium of the corpus callosum (SCC) [1]. On magnetic resonance imaging (MRI), this lesion resolves completely within a few weeks. The lesions typically appear in the central splenium [2].
Imaging findings typically include hyperintensity on diffusion-weighted imaging (DWI), hypo-intensity on apparent diffusion coefficient (ADC) maps, hyperintensity on T2-weighted images, and absence of gadolinium contrast enhancement [3]. Lesions may be confined to the SCC, corresponding RESLES type 1. In other cases, the lesion extends beyond the splenium to involve the entire corpus callosum and adjacent white matter, defining RESLES type 2. Regardless of the extent, these lesions usually resolve within 2 weeks without residual signal abnormalities or atrophy. Although diffusion restriction suggests cytotoxic edema, the reversible nature of the lesion and evidence from advanced neuroimaging support the interpretation that RESLES represents intramyelinic edema [2].
Adult-onset RESLES is relatively rare. It has been speculated that the characteristics of RESLES in adults are different from those in children. In this report, we present the largest series to date in our country of adult-onset RESLES cases occurring in distinct clinical settings, analyzing their presentation, clinical course, and outcomes compared to literature data on child-onset ones.
| Case Reports | ▴Top |
Methods
The subjects were inpatients at a university-affiliated tertiary care hospital in Marrakesh, Morocco, between June 2021 and November 2025. Potential cases of RESLES were identified through a systematic review of inpatient neurological and neuroimaging records. The diagnosis of RESLES was established based on characteristic neuroimaging findings. The medical history of each patient was reviewed. Information was collected including demographics, clinical characteristics, laboratory results, imaging findings, possible precipitating factors, treatments, and follow-up results.
Results
Clinical evaluation
Five patients (two males and three females) were retrospectively evaluated in this study. Subjects’ age varied between 29 and 46 years (average 33 ± 7.32 years). Most common neurological manifestations were headache (3/5), drowsiness (2/5), and slurred speech (2/5). Less common symptoms were hearing loss (1/5), blurred vision (1/5), dysarthria (1/5), limb ataxia (1/5), postural tremors (1/5), insomnia (1/5), and agitation (1/5). One patient presented fever prior to neurological symptoms and one patient had a single self-limiting seizure after which they were completely asymptomatic thereafter, aside from associated polyarthralgia and marked left hip pain.
Laboratory and CSF results
Among the patients, only one (1/5) had a confirmed infectious etiology, testing positive for Mycoplasma pneumoniae. Laboratory analysis revealed elevated white blood cell and neutrophils counts in three patients (3/5), along with increased C-reactive protein (CRP) levels (3/5) and erythrocyte sedimentation rate (2/5). Hematologic abnormalities included anemia in three patients (3/5), hypochromic microcytic in one (1/5) and normochromic normocytic in two (2/5), as well as leukopenia (1/5) and thrombocytopenia (2/5). Serum sodium levels were within normal limits in all cases; however, two patients exhibited mild hypokalemia, with potassium levels of 2.64 and 2.93 mmol/L, respectively. Elevated creatinine and blood urea nitrogen levels were observed in two patients (2/5). Screening for human immunodeficiency virus (HIV), hepatitis B virus (HBV), hepatitis C virus (HCV), and syphilis was negative in all subjects. Cerebrospinal fluid (CSF) analysis was normal in all five patients, although CSF opening pressure was elevated in one case (1/5). In one patient, muscle biopsy revealed malignant cell infiltration consistent with Burkitt lymphoma.
MRI findings
MRI examinations were performed between 7 and 20 days after the onset of prodromal symptoms. The imaging findings were variable among the five patients: three (3/5) exhibited RESLES type 1, lesions confined to the SCC, while two (2/5) showed RESLES type 2 lesions extending slightly beyond the SCC. SCC lesions demonstrated homogeneous diffusion restriction, appearing hyperintense on DWI and hypointense on ADC maps in all five cases. Additionally, the lesions were homogeneously isointense to mildly hyperintense on T2-weighted and fluid-attenuated inversion recovery (FLAIR) sequences, and isointense to hypointense on T1-weighted images (Fig. 1).
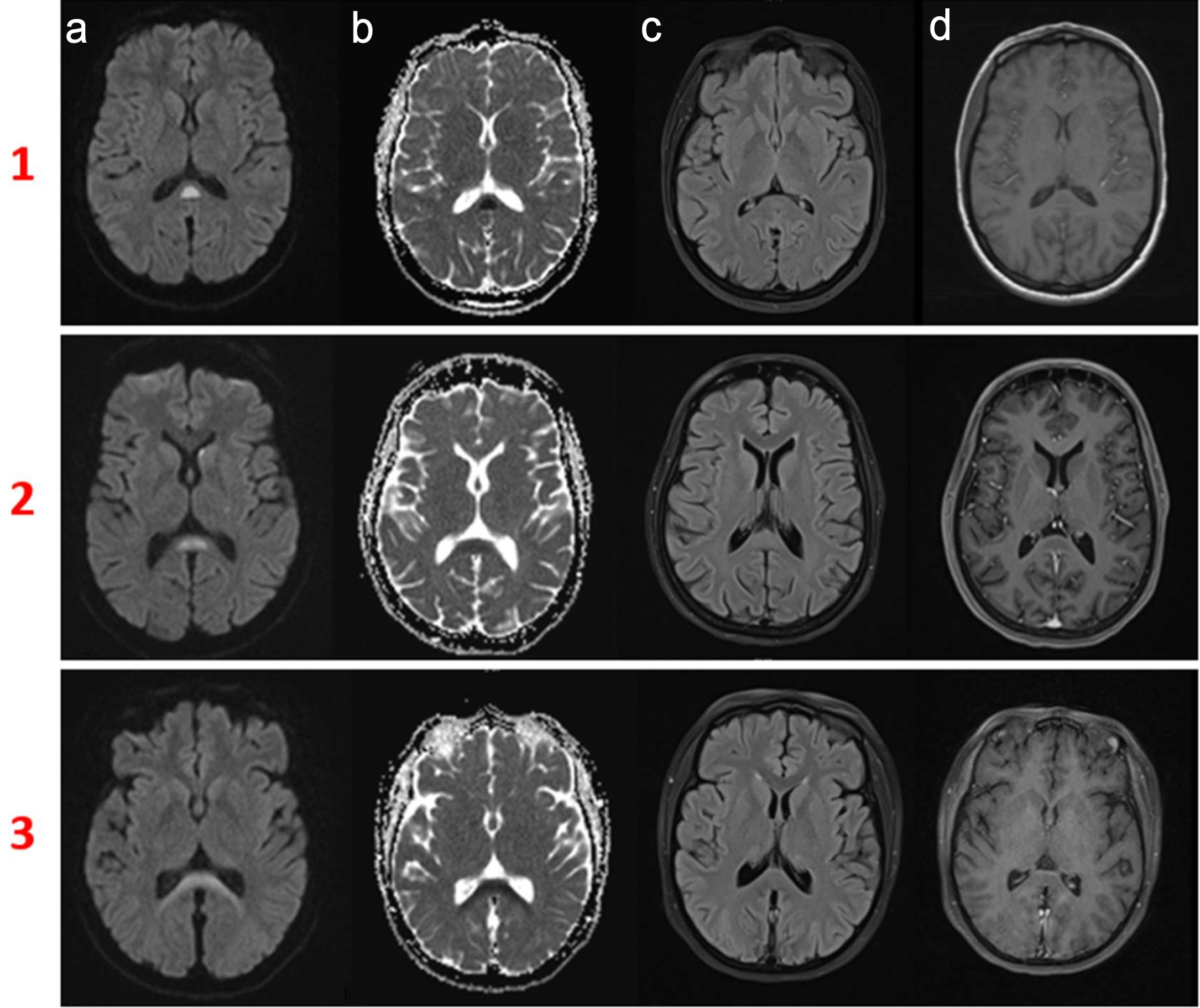 Click for large image | Figure 1. Magnetic resonance imaging (MRI) findings of reversible splenial lesion syndrome (RESLES) in adult cases. Rows 1 and 2 (cases 2 and 4 respectively): RESLES type 1, characterized by a lesion confined to the splenium of the corpus callosum (SCC). (a) Diffusion-weighted imaging (DWI) hyperintensity. (b) Corresponding apparent diffusion coefficient (ADC) hypo-intensity, consistent with restricted diffusion. (c, d) Hyperintensity on T2/FLAIR sequences and lack of enhancement post-gadolinium (d). Row 3 (case 5): RESLES type 2, showing the lesion extending from the SCC into the adjacent white matter with no evidence of central nervous system infiltration of Burkitt lymphoma. All lesions exhibited homogeneous hyperintensity on DWI and hypo-intensity on ADC maps, and fully resolved at follow-up. |
Therapy and follow-up
Clinical symptoms improved with symptomatic management and treatment of the underlying causes. None of the patients received intravenous corticosteroids nor intravenous immunoglobulin (IVIG). The follow-up period ranged from 2 to 30 months. Case 1 improved clinically within 1 week of anti-infectious therapy and experienced progressive recovery of hearing, which fully normalized within 10 months. Case 2 underwent ventriculoperitoneal shunt placement and anticoagulant therapy, resulting in marked clinical improvement. Case 3 received blood transfusion and hemodialysis, along with dual antibiotic therapy, and cerebellar symptoms resolved within 1 month. Case 4 was treated with risperidone, and complete clinical recovery was observed at the 2 months follow-up. Case 5 did not require specific neurological treatment, as the patient remained neurologically asymptomatic throughout. At the time of writing, the patient was undergoing intensive combination chemotherapy targeting Burkitt lymphoma. Table 1 summarizes clinical and radiological data of the five cases with clinical outcome.
 Click to view | Table 1. Summary of Clinical Presentations, Underlying Causes, MRI Features, Therapy, and Outcome of the Five Adult-Onset RESLES Cases |
| Discussion | ▴Top |
RESLES is a clinical condition involving transient lesions in the SCC. It was first reported by Kim and colleagues in 1999, describing lesions of the SCC concomitant with epilepsy and anti-epileptic medication use [4]. However, as increasing numbers of cases of RESLES have been reported, the lesion has been found to be associated with various other diseases and conditions. Adult-onset RESLES is relatively rare and it has been speculated that the characteristics of RESLES in adults are different from that in children. Many child-onset RESLES cases have been reported in Asia, especially Japan [5]. Similarly, most adult-onset RESLES cases have also been reported in Asia, including Japan, China, and India [3]. In a series of 130 children [6], RESLES was found to more likely occur in younger children under 3 years old, since this subgroup has immature and incomplete myelination [6]. In addition to this, infants and young children are more susceptible to infection which is a prominent cause of RESLES.
In children, the most commonly reported precipitating factor is infection, particularly gastrointestinal and respiratory infections, with rotavirus and Mycoplasma pneumoniae being the primary agents [6]. In adults, published cases suggest that RESLES may be triggered by a wider range of infectious pathogens, including viral infections such as influenza and human herpesvirus [3], as well as bacterial infections, most notably Mycoplasma pneumoniae [7]. Neurological involvement is a common extrapulmonary manifestation of Mycoplasma pneumoniae infection [7]. Our first case illustrates a typical presentation of adult-onset RESLES secondary to a Mycoplasma pneumoniae respiratory infection. Adult-onset RESLES has been reported mainly in association with epilepsy and antiepileptic drug use [3]. Other documented causes include substance withdrawal, metabolic disturbances, drug-related toxicity, malignancy, cerebrovascular disease, traumatic brain injury, status migrainosus, and high-altitude exposure [7, 8]. In our series, the etiologies were diverse ranging from the postpartum state and cerebral venous thrombosis (CVT) to lymphoma, multiple organ failure, renal failure, and hypokalemia, highlighting the broader spectrum of triggers in adults compared with pediatric-onset cases. Regarding the postpartum period, RESLES has been described in association with preeclampsia, CVT, postpartum cerebral angiopathy, and reversible cerebral vasoconstriction syndrome (RCVS) [8, 9]. Only a few published cases describe RESLES occurring in an otherwise uncomplicated peri- or postpartum period, similar to our fourth case [9, 10]. Reports of concomitant CVT and RESLES are likewise limited, with the postpartum state frequently identified as a contributing factor [9]. To our knowledge, no previous cases of RESLES associated with lymphoma have been reported, making our fifth case the first described in this context.
Clinically, seizure was the most common presenting symptom among children, along with disturbance of consciousness and other neurological symptoms [3]. In adults, the most common neurological manifestations of RESELS were headache and disturbance of consciousness [2]. In our series, the most common symptoms were headache and drowsiness. Clinical manifestations of reversible splenial lesions in adults are nonspecific and variable, often mimicking encephalopathy or encephalitis. The most common prodrome is fever, frequently accompanied by headache and gastrointestinal symptoms [7, 8]. Neurological features may include cognitive impairment, seizures, behavioral changes, confusion, drowsiness, delirium, and acute urinary retention. Less common but reported symptoms are motor decline, slurred speech, neck stiffness, coma, tremor, ataxia, somnolence, dysarthria, visual disturbances, and dizziness [2]. The most uncommon symptom in our series was perceptive hearing loss; however, disturbance of the callosal pathways may result in deficits affecting motor control, spatial orientation, visual and auditory processing, as well as language-related behaviors [8], which could explain the auditory involvement in our case.
Several hypotheses have been proposed to explain the genesis of splenial lesions in the SCC. Tada et al speculated that intramyelinic edema and inflammatory cell infiltration were key mechanisms. According to this hypothesis, the edema and diffusion restriction observed in reversible splenial lesions result from excitotoxicity driven by elevated extracellular glutamate. Glutamate binding to non–N-methyl-D-aspartate (non-NMDA) receptors promotes sodium influx, leading to cytotoxic edema. However, the identification of a similar splenial lesion in a neonate with incomplete myelination challenges this view and suggests that intramyelinic edema alone may not fully account for the condition. Additional proposed mechanisms include immune system activation, oxidative stress, and disturbances in fluid balance. In children, since infection is the most common triggering factor, some authors have speculated that a distinctive post-infectious inflammatory mechanism indirectly leads to splenial lesions [6], particularly because pathogens are rarely detected in the CSF. Therefore, the pathogenesis of RESLES may differ between adult and pediatric populations.
RESLES is generally of a favorable prognosis. Evidence supporting the efficacy of methylprednisolone pulse therapy or IVIG in the management of RESLES remains limited [3]. In a literature review published in 2017 that included 15 adult case reports [3], only seven patients received either methylprednisolone pulse therapy or IVIG. Notably, the clinical outcomes of treated patients were comparable to those who did not receive these interventions; all patients recovered completely regardless of therapy. In pediatric populations, although methylprednisolone pulse therapy and IVIG have been recommended for infectious encephalopathy irrespective of the causative pathogen or clinico-radiological syndrome, robust evidence for their effectiveness in RESLES is still lacking; however, children presenting with more severe clinical symptoms or extensive radiological involvement may require prolonged hospitalization and are at greater risk of developing neurological sequelae [5]. The largest pediatric case series to date [6] reported that the vast majority of patients recovered fully without steroid therapy. Only nine children out of 130 received intravenous dexamethasone, and all children exhibited normal neurodevelopment [6]. These observations suggest that corticosteroids and IVIG may not be essential for recovery and that RESLES often follows a self-limiting course in both adults and children. Furthermore, the absence of significant differences in prognosis between treated and untreated patients indicates that supportive and etiological management alone may be sufficient in most cases. This suggests that most RESLES cases, regardless of age group, clinical manifestation, or underlying cause, can be effectively managed without aggressive therapy.
Conclusion
RESLES is a clinico-radiological syndrome with a wide variety of etiologies. Infection appears to be the most common cause in children. While epilepsy and antiepileptic drugs were historically considered the primary triggering factors in adults, a multitude of other causes have been identified recently. Infants are more likely to present with seizures, whereas older populations tend to exhibit disturbances of consciousness, headaches, dizziness, and other more complex neurological symptoms. Radiological features are consistent across all age groups, and follow-up data suggest that management does not require population-specific differences.
Acknowledgments
We would like to express our gratitude to the staff of the Neurology Department at Mohammed VI University Hospital in Marrakesh for their support and the care provided to each and every patient of this series.
Financial Disclosure
No funding sources or financial support were received for the paper.
Conflict of Interest
No potential conflicts of interest related to the paper or the authors.
Informed Consent
Written informed consent was obtained from all five patients, or their legally authorized representatives, for the publication of this case series, including the clinical details and accompanying images.
Author Contributions
Conception and design: Khaoula Belaidi. Supervision: Safae Zahlane. Cases study: Khaoula Belaidi, M’Hamed Riad Amanallah, Oumayna Azzou, and Hamza Benzakour. Literature review: Khaoula Belaidi. Writer: Khaoula Belaidi. Critical review: Nissrin Louhab, Mohamed Chraa, and Yasmina Zakaria.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
ADC: apparent diffusion coefficient; CSF: cerebrospinal fluid; CVT: cerebral venous thrombosis; DWI: diffusion-weighted imaging; HBV: hepatitis B virus; HCV: hepatitis C virus; HIV: human immunodeficiency virus; IVIG: intravenous immunoglobulin; MRI: magnetic resonance imaging; non-NMDA: non–N-methyl-D-aspartate; RCVS: reversible cerebral vasoconstriction syndrome; RESLES: reversible splenial lesion syndrome; SCC: splenium of the corpus callosum
| References | ▴Top |
- Tetsuka S. Reversible lesion in the splenium of the corpus callosum. Brain Behav. 2019;9(11):e01440.
doi pubmed - Zhang Z, Guo J, Li X, Li C, Ma X, Cui X. Mild encephalitis/encephalopathy with a reversible isolated splenial lesion (MERS) in adult patients: a small case series. Eur Neurol. 2020;83(3):279-286.
doi pubmed - Yuan J, Yang S, Wang S, Qin W, Yang L, Hu W. Mild encephalitis/encephalopathy with reversible splenial lesion (MERS) in adults-a case report and literature review. BMC Neurol. 2017;17(1):103.
doi pubmed - Kun L, et al. Drug toxicity? Callosum in epileptic patients: antiepileptic focal lesion in the splenium of the corpus focal lesion in the splenium of the corpus callosum in epileptic patients: antiepileptic drug toxicity? 1999. [Online]. Available: http://www.ajnr.org/content/20/1/.
- Chen WX, Liu HS, Yang SD, Zeng SH, Gao YY, Du ZH, Li XJ, et al. Reversible splenial lesion syndrome in children: retrospective study and summary of case series. Brain Dev. 2016;38(10):915-927.
doi pubmed - Chen H, Yu X, Chen Y, Wu H, Wu Z, Zhong J, Tang Z. Reversible splenial lesion syndrome in children: a retrospective study of 130 cases. Front Neurol. 2023;14:1241549.
doi pubmed - Dong X, Cong S. Reversible splenial lesion syndrome associated with acute Mycoplasma pneumoniae-associated encephalitis: A report of four cases and literature review. Exp Ther Med. 2018;16(3):2152-2159.
doi pubmed - Tang Y, Zhang D, Ge J, Jin J, Liu Y, Chen S, He M. Clinical and imaging features of reversible splenial lesion syndrome with language disorder. Transl Neurosci. 2020;11(1):210-214.
doi pubmed - Mubasher M, Hanafi A, Schaeffer C, Alkhoury Z. A case of reversible splenial lesion syndrome in early post-partum period,” Interdiscip Neurosurg. 2019;17:7-9.
doi - Vold V, Tingvoll SH, Beyer MK, Nordengen K. Case report: re-evaluating reversibility of cytotoxic lesions of the corpus callosum. Front Neuroimaging. 2025;4:1436931.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Neurology Research is published by Elmer Press Inc.