| Journal of Neurology Research, ISSN 1923-2845 print, 1923-2853 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Neurol Res and Elmer Press Inc |
| Journal website https://jnr.elmerpub.com |
Original Article
Volume 16, Number 1, March 2026, pages 30-39

The Role of Calcitriol (Vitamin D) as Neuroprotection and Prognostic Biomarker in Patients With Ischemic and Hemorrhagic Stroke
I Nyoman Windianaa, d, Luh Putu Lina Kameliab, I. Nyoman Gede Narendra Yanakusumac, Luh Made Karuni Kartika Saria
aFaculty of Medicine, Universitas Pendidikan Ganesha, Bali, Indonesia
bDepartment of Neurology, Faculty of Medicine, Universitas Pendidikan Ganesha, Bali, Indonesia
cFaculty of Medicine, Universitas Udayana, Bali, Indonesia
dCorresponding Author: I Nyoman Windiana, Faculty of Medicine, Universitas Pendidikan Ganesha, Bali, Indonesia
Manuscript submitted December 17, 2025, accepted January 30, 2026, published online March 13, 2026
Short title: Vitamin D in Stroke: Neuroprotection & Prognosis
doi: https://doi.org/10.14740/jnr1089
| Abstract | ▴Top |
Background: Stroke is a leading cause of long-term neurological disability, significantly impacting global morbidity and mortality. Vitamin D supplementation shows neuroprotective potential, yet research on its effects and role as a prognostic biomarker in stroke patients remains limited.
Methods: This systematic review and meta-analysis followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We searched Google Scholar, PubMed, and Scopus for studies assessing vitamin D’s neuroprotective effects, measured by standardized mean difference (SMD) with a 95% confidence interval (CI). We also evaluated vitamin D levels as a biomarker for stroke prognosis using odds ratio (OR) with a 95% CI. Out of 3,171 identified articles, 23 relevant studies involving 4,911 patients with ischemic and hemorrhagic strokes were included.
Results: The analysis indicated that vitamin D supplementation significantly improved neurological function (SMD, 0.63; 95% CI, 0.31–0.95; P = 0.0001) for both high-dose intramuscular injections and low-dose oral supplementation given daily or weekly. Additionally, low vitamin D levels were associated with stroke severity (OR, 3.44; 95% CI, 1.84–6.44; P < 0.0001), suggesting that vitamin D levels have potential as a prognostic biomarker.
Conclusion: These findings underscore the importance of vitamin D as an additional therapeutic strategy in stroke management. Despite the heterogeneity in the analysis, the results support the need for further research to determine the optimal dosage and to understand the effects of comorbidities. Additionally, the development of evidence-based clinical practice guidelines is necessary for the implementation of vitamin D administration in stroke rehabilitation.
Keywords: Vitamin D; Calcitriol; Neuroprotection; Stroke
| Introduction | ▴Top |
As one of the most urgent medical conditions, stroke is a leading cause of neurological disability and a major contributor to global morbidity and mortality, requiring substantial attention in both research and preventive strategies. According to the World Health Organization (WHO), stroke was the third leading cause of death and disability worldwide in 2021, with 11.9 million new cases and 93.8 million people living with stroke globally [1]. Epidemiological data further demonstrate the substantial burden of cerebrovascular disease. The cumulative incidence of stroke has been reported as 218 per 100,000 population in males (95% confidence interval (CI), 214–221) and 127 per 100,000 in females (95% CI, 125–128), highlighting significant sex-related differences in stroke incidence [2]. Stroke remains a major cause of death and long-term disability worldwide, underscoring the urgent need for effective preventive and therapeutic interventions [3].
One intervention of particular interest is vitamin D supplementation, which has been increasingly recognized for its potential neuroprotective effects [3]. Vitamin D is involved in modulating cognitive function, neurotrophic signaling pathways, and mechanisms that reduce oxidative stress and inflammation processes that play a critical role in neuronal injury following stroke [4]. Notably, the prevalence of vitamin D deficiency has been reported to reach up to 71% among stroke patients and has been associated with greater stroke severity and poorer functional outcomes [5, 6]. Therefore, this study aims to evaluate the neuroprotective effects of vitamin D supplementation and its potential role as a prognostic biomarker in patients with ischemic and hemorrhagic stroke.
| Materials and Methods | ▴Top |
Study design
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. To ensure methodological transparency and integrity, the study has been registered with PROSPERO under registration number CRD42024600826, indicating that the protocol for this systematic review has been documented and verified.
Research ethics
As this study is a systematic review and does not involve the collection of primary data from human subjects, ethical approval from a review board was not necessary.
Data sources and literature search
Two independent reviewers conducted the article search using Google Scholar, PubMed, and Scopus databases. The search included all articles published from the inception of each database up to September 23, 2024. The search terms used were (“vitamin D” OR “calcitriol”) AND (“neuroprotective effect” OR “neuroprotection” OR “neuroprotective efficacy”) AND (“stroke” OR “ischemic stroke” OR “hemorrhagic stroke”). This search was limited to studies evaluating the neuroprotective effects and potential prognostic value of vitamin D in patients with ischemic and hemorrhagic stroke (Fig. 1).
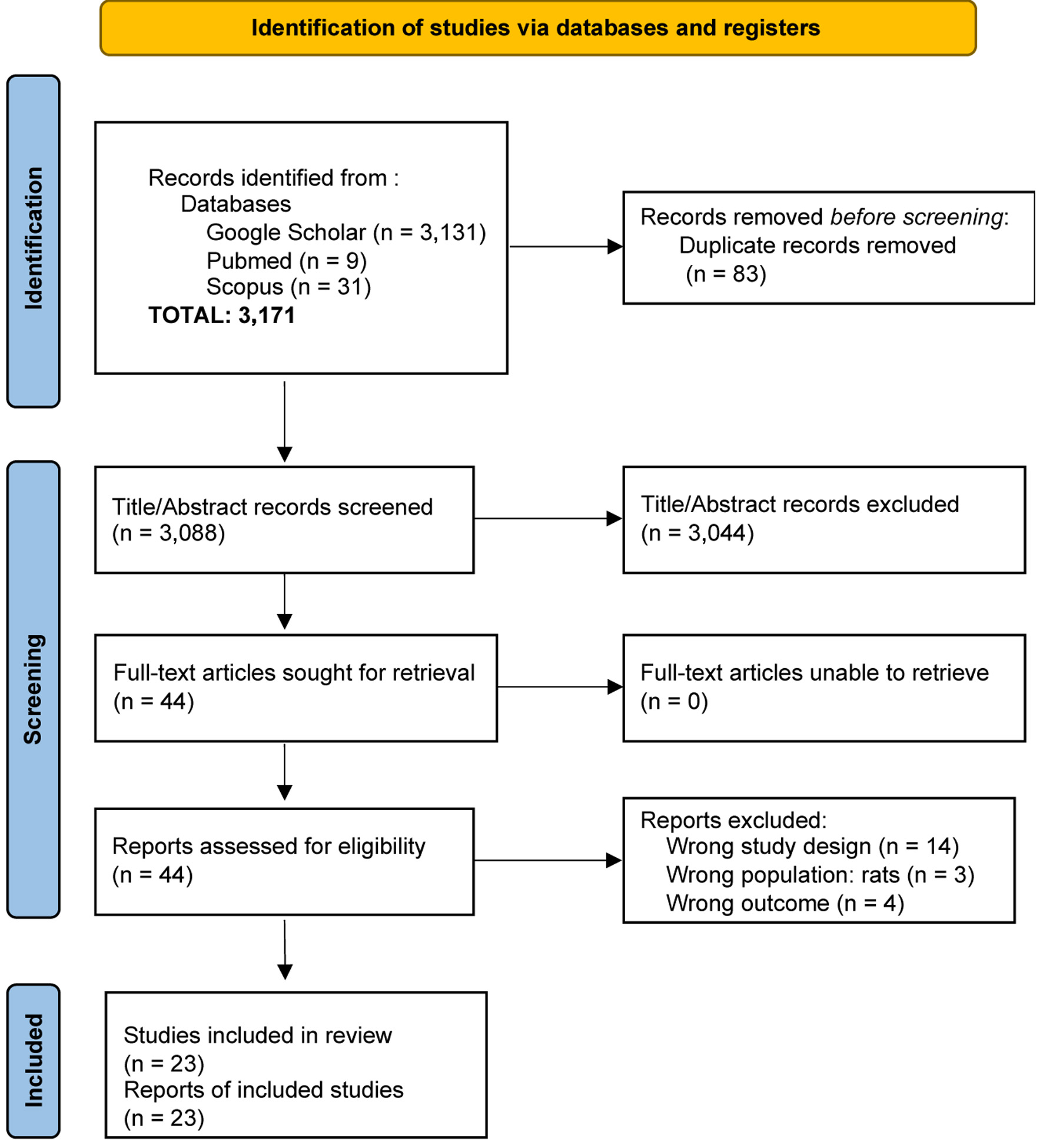 Click for large image | Figure 1. Flow diagram of the study selection process for articles included in the systematic review and meta-analysis. |
Study selection criteria and quality assessment
The inclusion criteria for this study were established based on the following conditions: 1) adult patients suffering from ischemic or hemorrhagic stroke, with a National Institutes of Health Stroke Scale (NIHSS) score greater than 5, confirmed by findings of infarction or hemorrhage in the brain identified by a neurologist through computed tomography; 2) one episode of focal neurological deficit with acute onset, lasting more than 24 h; 3) patients admitted within the last 24 h after being diagnosed with ischemic or hemorrhagic stroke and having vitamin D deficiency (serum 25-OH vitamin D ≤ 30 ng/mL). Patients were excluded from the study if they had a history of acute or chronic renal failure (creatinine clearance < 30 mL/min/1.73 m2), liver failure, secondary stroke due to neuroinfection, cancer, trauma, previous stroke, premorbid disability, or neurological disorders such as dementia, Alzheimer’s disease, multiple sclerosis, or Parkinson’s disease. Two authors independently reviewed the titles and abstracts. In cases of disagreement between reviewers, consultation was conducted to reach a final decision. The risk of bias was assessed using the Cochrane risk of bias 2 (ROB-2) tool for studies with a randomized controlled trial design to evaluate the methodological quality of the eligible articles. Additionally, the risk of bias in non-randomized studies of interventions (ROBINS-I) tool was used to assess the risk of bias in the effectiveness or safety (benefit or harm) of interventions in non-randomized studies. Any discrepancies in data extraction or quality assessment were resolved through discussion.
Data extraction
Two independent authors performed the data extraction process. Data collection was conducted by organizing the following variables: first author, year of publication, study location, sample size, study design, diagnosis, stroke assessment, serum vitamin D levels, intervention regimen, control regimen, and tools for assessing neurological clinical improvement.
Outcomes
The primary outcome of this meta-analysis was neurological function improvement following vitamin D supplementation. Neurological function was assessed using validated clinical scales, including NIHSS, Barthel Index (BI), Scandinavian Stroke Scale (SSS), Brunnstrom Recovery Stage (BRS), Functional Ambulation Classification (FAC), modified Rankin Scale (mRS), Functional Independence Measure (FIM), Mini-Mental State Examination (MMSE), Montgomery-Åsberg Depression Rating Scale (MADRS), and Neuron-Specific Enolase (NSE).
Secondary outcomes included the association between serum vitamin D levels and stroke severity, which was evaluated to explore the potential role of vitamin D as a prognostic biomarker.
Statistical analysis
We conducted a meta-analysis to evaluate the study outcomes. The effect of vitamin D supplementation on neurological function as a neuroprotective agent was measured using the standardized mean difference (SMD) with a 95% CI. For dichotomous data, specifically the assessment of vitamin D levels as a biomarker for stroke prognosis, we used the odds ratio (OR) with a 95% CI. Heterogeneity among studies was assessed using the I2 statistic, with 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. Statistical significance was set at a P-value of ≤ 0.05. In cases of moderate to high heterogeneity, a random-effects model was applied to the meta-analysis; otherwise, a fixed-effect model was used for low heterogeneity. All statistical analyses were performed using Review Manager 5.1.0, developed by Cochrane, UK.
| Results | ▴Top |
Article search and selection
A total of 3,171 potential research articles were identified. After removing duplicates, screening, conducting full-text reviews, and applying the inclusion and exclusion criteria, 23 relevant articles were selected for the systematic review and meta-analysis (Fig. 1).
Risk of bias assessment
Based on the ROB-2 assessment, which evaluates the quality of research on primary outcomes, two of the seven articles included in this study raised concerns regarding bias. These articles were authored by Karasu et al (2021) [7] and Narasimhan et al (2017) [8]. According to the ROBINS-I assessment, which evaluates the quality of research on secondary outcomes, 10 out of the 16 articles included in this study exhibited a moderate risk of bias. These articles were authored by Afshari et al (2015) [9], Aggarwal et al (2022) [10], Alfieri et al (2017) [11], Borowicz et al (2023) [12], Rad et al (2021) [13], Samarakoon et al (2024) [14], Turetsky et al (2015) [15], Wajda et al (2019) [16], Kim et al (2020) [17], and Park et al (2015) [18]. Figure 2 presents the evaluation of bias risk.
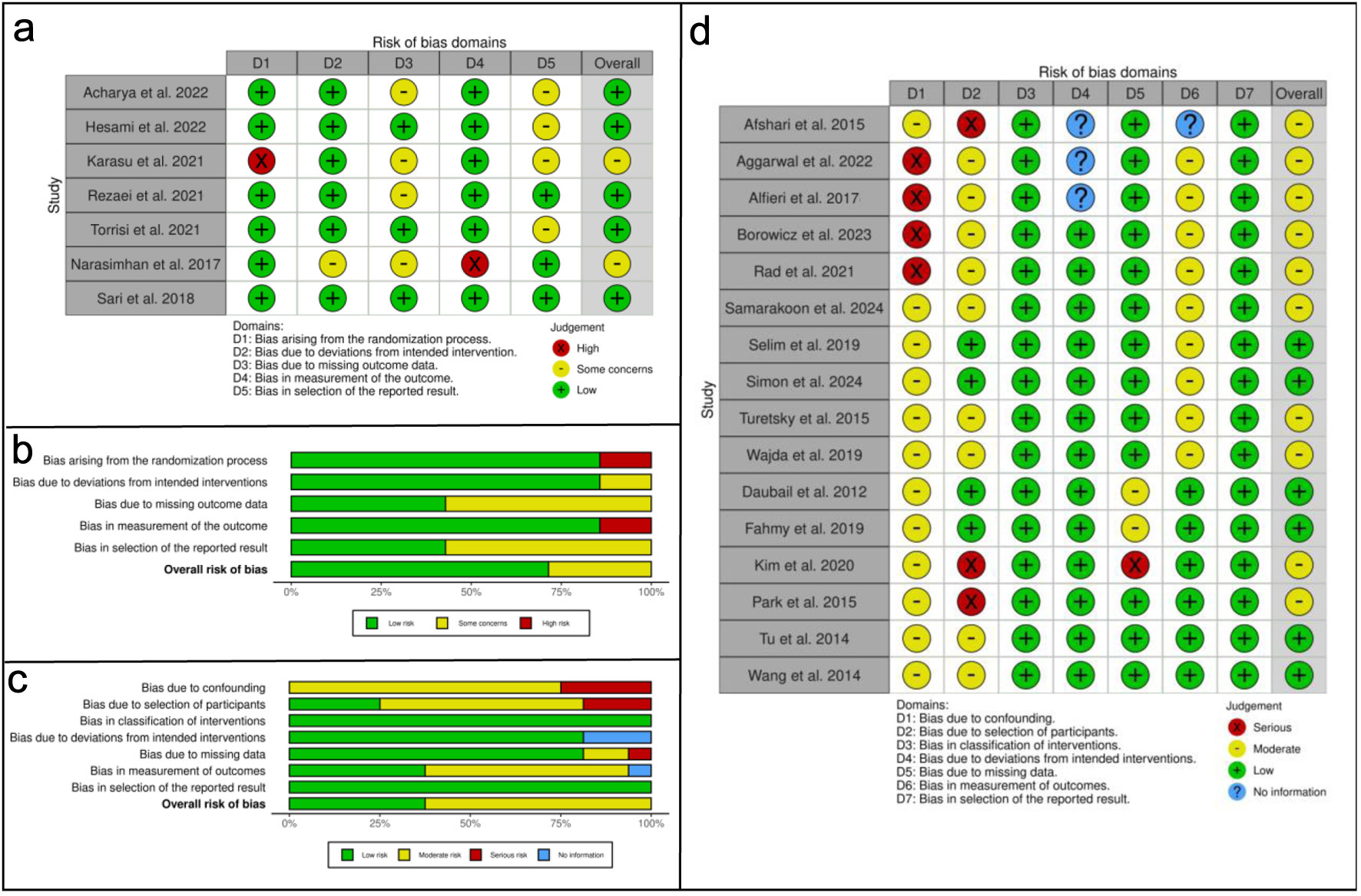 Click for large image | Figure 2. Risk of bias analysis. (a) Traffic-light plot of the risk of bias assessment using ROB-2, illustrating the bias risk results for the effect of vitamin D supplementation on neurological function improvement across each domain. (b) Overall risk of bias conclusion using ROB-2, summarizing the risk of bias regarding the effect of vitamin D supplementation on neurological function improvement. (c) Overall risk of bias conclusion using ROBINS-I, indicating the risk of bias for vitamin D levels as a prognostic biomarker in stroke severity. (d) Traffic-light plot of the risk of bias assessment using ROBINS-I, depicting the risk of bias for the analysis of vitamin D levels in stroke severity as a prognostic biomarker across each domain. ROB-2: risk of bias 2; ROBINS-I: risk of bias in non-randomized studies of interventions. |
Study characteristics
Tables 1 and 2 provide a comprehensive overview of the studies included in this analysis. A total of 23 studies involving 4,911 stroke patients (both ischemic and hemorrhagic strokes) were published between 2014 and 2024. The sample sizes varied across studies, ranging from 40 to 818 stroke patients.
 Click to view | Table 1. Characteristics of Study Data on Primary Outcome (Effect of Vitamin D Supplementation on Neurological Function Improvement) |
Click to view | Table 2. Characteristics of Study Data on Secondary Outcome (Analysis of Vitamin D Levels in Stroke Severity as a Prognostic Biomarker) |
Meta-analysis results
Effect of vitamin D supplementation on neurological function improvement
Seven studies were included in the analysis to evaluate the effect of vitamin D supplementation on neurological function (Fig. 3a). Based on the heterogeneity test (I2 = 60%), the SMD for the effect of vitamin D supplementation on neurological function was analyzed using a random-effects model. Statistical analysis revealed that vitamin D supplementation significantly improved neurological function compared to the control group (SMD, 0.63; 95% CI, 0.31–0.95; P = 0.0001). Both low-dose oral daily and weekly administration (SMD, 0.91; 95% CI, 0.25–1.59; P = 0.007) and a single high-dose intramuscular injection (SMD, 0.52; 95% CI, 0.18–0.55; P = 0.002) were effective in enhancing neurological function.
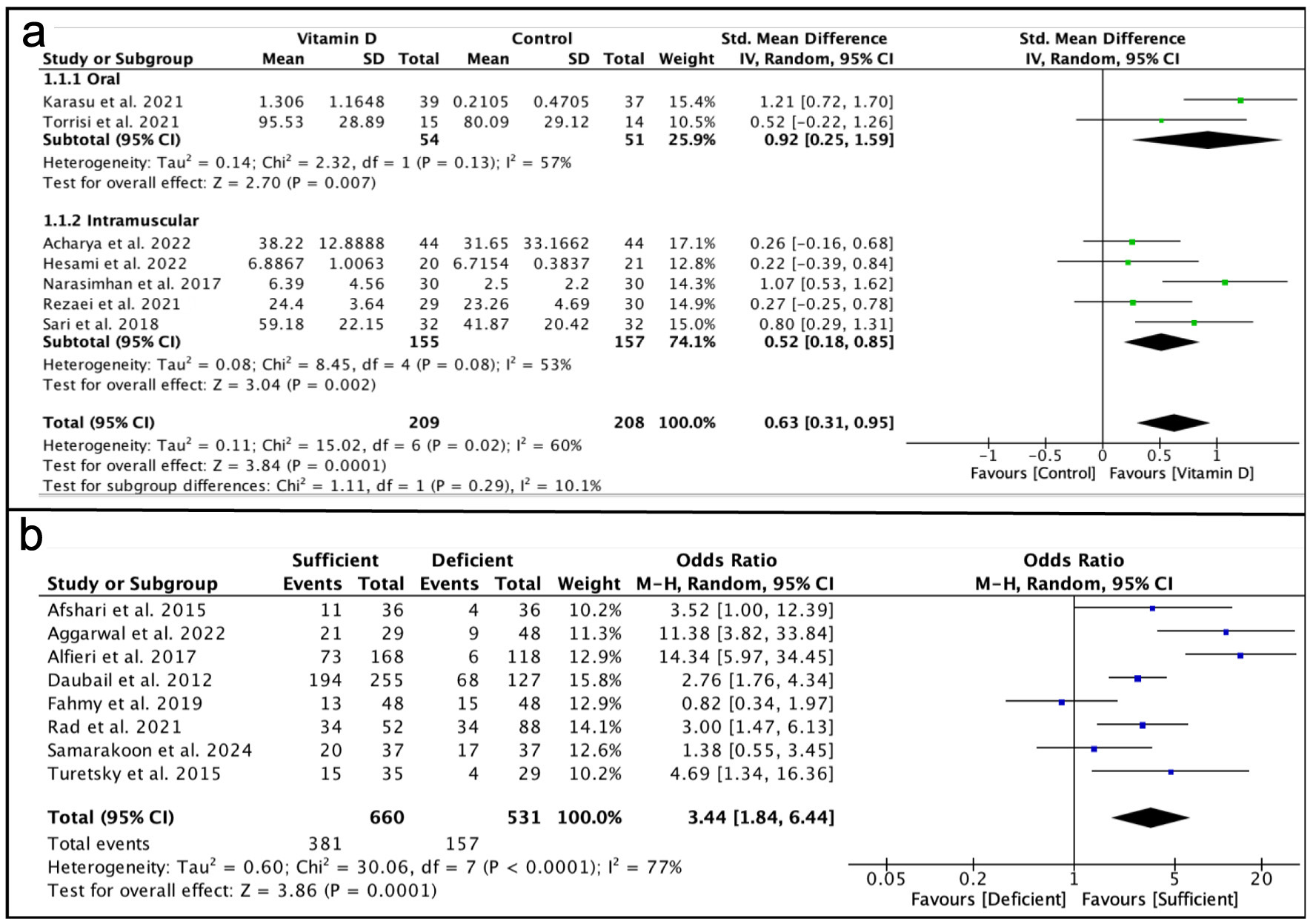 Click for large image | Figure 3. Analysis results. (a) Forest plot showing the effect of vitamin D supplementation on neurological function improvement compared to the control group. (b) Forest plot analyzing vitamin D levels in relation to stroke severity as a prognostic biomarker. |
Vitamin D levels in stroke severity as a prognostic biomarker
Eight studies were included in the analysis of vitamin D levels in relation to stroke severity as a prognostic biomarker (Fig. 3b). Based on the heterogeneity test (I2 = 77%), the OR for the prognostic biomarker value was pooled using a random-effects model. Statistical analysis indicated that low vitamin D levels in stroke patients were associated with increased severity of neurological dysfunction compared to the control group (OR, 3.44; 95% CI, 1.84–6.44; P < 0.0001).
Publication bias assessment
The analysis revealed a heterogeneity I2 value of 60% for the primary outcomes and 77% for the secondary outcomes, indicating moderate heterogeneity among the included studies. This suggests that the study findings exhibit some variation or inconsistency, which may be attributed to differences in study design, population, interventions, or measurement tools used to assess improvements in neurological function. To evaluate the potential for publication bias in the primary and secondary outcome meta-analyses, we used the funnel plot function of meta-bias from Review Manager 5.1.0, Cochrane, UK. Upon examination of the funnel plot, it was challenging to determine whether the distribution of studies on both sides of the plot was symmetric, as there were fewer than 10 studies included for each outcome. This suggests that the potential for publication bias could not be reliably assessed.
| Discussion | ▴Top |
The aim of this systematic review and meta-analysis was to evaluate the role of vitamin D in neuroprotective effects and its potential as a prognostic biomarker for stroke severity. Data analysis showed that vitamin D supplementation led to a significant improvement in neurological function compared to the control group (SMD, 0.63; 95% CI, 0.31–0.95; P = 0.0001). This improvement was observed with both high-dose single intramuscular injections (SMD, 0.52; 95% CI, 0.18–0.85; P = 0.002) and low-dose oral supplementation administered daily or weekly (SMD, 0.92; 95% CI, 0.25–1.59; P = 0.007) in patients with ischemic and hemorrhagic stroke.
Administering a single high-dose intramuscular injection of vitamin D to ischemic and hemorrhagic stroke patients may be a viable supplementation option, particularly for those with low adherence to daily or weekly oral treatments [19, 20]. Furthermore, a high-dose single injection can rapidly and safely increase serum 25-OH vitamin D levels [21–23]. The analysis also indicated that adequate vitamin D levels in stroke patients are associated with better prognosis regarding neurological function improvement compared to low vitamin D levels (OR, 3.44; 95% CI, 1.84–6.44; P < 0.0001). Our analysis suggests that daily and weekly vitamin D doses, totaling between 200,000 and 600,000 IU, can enhance neurological function in ischemic and hemorrhagic stroke patients, as assessed by SSS, mRS, NIHSS, and BI scores. Additionally, a single intramuscular injection of vitamin D at doses between 300,000 and 600,000 IU demonstrated significant improvements in neurological function.
It is important to note that the inflammatory process plays a crucial role in stroke pathogenesis [24]. The anti-inflammatory effects of vitamin D have been demonstrated in various diseases, such as multiple sclerosis (MS) and epilepsy [25]. The neuroprotective mechanisms induced by vitamin D are complex, involving the inhibition of the prostaglandin (PG) and cyclooxygenase-2 (COX-2) pathways, a reduction in matrix metalloproteinase-9 (MMP-9), and an increase in anti-inflammatory cytokines [26]. Deficiency in 25-hydroxyvitamin D (25(OH)D) can lead to prolonged immune-inflammatory responses, reducing neuroprotection and resulting in a poor prognosis for stroke patients [27]. Therefore, adequate vitamin D levels may serve as a protective factor against ischemic reperfusion injury in stroke cases, as well as offering protective effects against neurovascular injury [28]. Low serum vitamin D levels have been associated with an increased risk of stroke and poor stroke prognosis [29]. Poor vitamin D status in stroke patients is also closely linked to an elevated risk of future cerebrovascular incidents [30, 31].
Limitations
Several limitations of this study should be acknowledged. First, the included studies varied in design, encompassing both randomized controlled trials and non-randomized studies, which may have affected the consistency of the findings and increased the risk of bias. Additionally, moderate heterogeneity was observed, with I2 values reaching 63% for primary outcomes and 71% for secondary outcomes. This heterogeneity is likely attributable to differences in study populations, vitamin D dosages, and outcome assessment methods. Variability in serum vitamin D measurement techniques across studies may have further influenced the results and their interpretation.
Another important limitation relates to sex-specific differences in stroke. Most of the included studies did not provide sufficient sex-disaggregated data to allow subgroup or stratified analyses. Consequently, the potential influence of sex on the neuroprotective effects of vitamin D supplementation and its role as a prognostic biomarker could not be fully explored.
Furthermore, comorbid conditions such as diabetes mellitus and hypertension, which may influence both stroke outcomes and vitamin D metabolism, were not consistently reported across studies and therefore could not be analyzed in detail. In addition, emerging aspects such as the effects of vitamin D on cerebral white matter integrity, cognitive impairment, and clusters of silent vascular risk factors associated with aging could not be systematically evaluated due to limited and non-standardized reporting of neuroimaging, cognitive, and subclinical vascular data across the included studies.
Future research
In addition to the outcomes assessed in this study, emerging evidence suggests that vitamin D may play a role in cerebral white matter integrity and cognitive function, both of which are important determinants of long-term outcomes after stroke. Alterations in white matter structure and cognitive impairment have been associated with aging-related cerebrovascular pathology and may be influenced by clusters of silent vascular risk factors. Although these aspects are clinically relevant, they could not be systematically evaluated in the present meta-analysis due to the lack of standardized reporting and insufficient data across the included studies.
These limitations highlight important directions for future research. Well-designed, large-scale randomized controlled trials are needed to clarify the optimal dosage, timing, and route of vitamin D supplementation in both ischemic and hemorrhagic stroke populations. Furthermore, future studies should incorporate sex-specific analyses, neuroimaging markers of white matter changes, detailed cognitive assessments, and comprehensive evaluation of subclinical vascular risk factors to further elucidate the neuroprotective mechanisms of vitamin D and refine its role as a prognostic biomarker in stroke outcomes.
Conclusions
This systematic review and meta-analysis demonstrates that vitamin D supplementation is associated with improved neurological function in patients with ischemic and hemorrhagic stroke, using both oral and intravenous regimens. In addition, low serum vitamin D levels are associated with greater stroke severity, supporting the potential role of vitamin D as a prognostic biomarker.
Despite heterogeneity among the included studies and the limited availability of sex-specific and comorbidity-related data, these findings underscore the clinical relevance of vitamin D in stroke management. Further well-designed prospective studies are required to determine optimal supplementation strategies and to establish evidence-based recommendations for the use of vitamin D in stroke care.
Acknowledgments
The authors would like to express their sincere gratitude to the Faculty of Medicine, Universitas Pendidikan Ganesha, for their guidance and academic support during the preparation of this manuscript.
Financial Disclosure
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this article.
Informed Consent
Not applicable, as this study is a systematic review and meta-analysis of previously published data.
Author Contributions
I Nyoman Windiana conceived and designed the study, developed the research protocol, conducted literature search and study selection, performed data extraction and statistical analysis, and drafted the manuscript. Luh Putu Lina Kamelia contributed to literature search, study selection, data extraction, and critical revision of the manuscript for important intellectual content. I Nyoman Gede Narendra Yanakusuma participated in data extraction, quality assessment of included studies, and statistical analysis. Luh Made Karuni Kartika Sari contributed to data interpretation, manuscript editing, and critical review of the final version. All authors read and approved the final manuscript.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
BI: Barthel Index; BRS: Brunnstrom Recovery Stage; CI: confidence interval; COX-2: cyclooxygenase-2; FAC: Functional Ambulation Classification; FIM: Functional Independence Measure; I2: I-squared statistic; MADRS: Montgomery-Åsberg Depression Rating Scale; MMSE: Mini-Mental State Examination; mRS: modified Rankin Scale; MMP-9: matrix metalloproteinase-9; MS: multiple sclerosis; NIHSS: National Institutes of Health Stroke Scale; NSE: Neuron-Specific Enolase; OR: odds ratio; PG: prostaglandin; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PROSPERO: International Prospective Register of Systematic Reviews; ROB-2: risk of bias 2; ROBINS-I: risk of bias in non-randomized studies of interventions; SMD: standardized mean difference; SSS: Scandinavian Stroke Scale; WHO: World Health Organization; 25(OH)D: 25-hydroxyvitamin D
| References | ▴Top |
- World Health Organization. Stroke [Internet]. Geneva: World Health Organization; 2023 [cited Jan 28, 2026]. Available from: https://www.who.int/news-room/fact-sheets/detail/stroke.
- Marrugat J, Arboix A, Garcia-Eroles L, Salas T, Vila J, Castell C, Tresserras R, et al. [The estimated incidence and case fatality rate of ischemic and hemorrhagic cerebrovascular disease in 2002 in Catalonia]. Rev Esp Cardiol. 2007;60(6):573-580.
doi pubmed - Ashouri R, Fangman M, Brielmaier J, Fields ZA, Campo N, Dore S. Nutritional supplementation of naturally occurring vitamin D to improve hemorrhagic stroke outcomes. Front Neurol. 2021;12:670245.
doi pubmed - Rihal V, Khan H, Kaur A, Singh TG. Vitamin D as therapeutic modulator in cerebrovascular diseases: a mechanistic perspectives. Crit Rev Food Sci Nutr. 2023;63(25):7772-7794.
doi pubmed - Zeng YY, Yuan CX, Wu MX, Cheng L, Zhou SN, Hu PL, Fan KL, et al. Low vitamin D levels and the long-term functional outcome of stroke up to 5 years. Brain Behav. 2021;11(10):e2244.
doi pubmed - Cui P, Hou H, Song B, Xia Z, Xu Y. Vitamin D and ischemic stroke - Association, mechanisms, and therapeutics. Ageing Res Rev. 2024;96:102244.
doi pubmed - Utkan Karasu A, Kaymak Karatas G. Effect of vitamin D supplementation on lower extremity motor function and ambulation in stroke patients. Turk J Med Sci. 2021;51(3):1413-1419.
doi pubmed - Narasimhan S, Balasubramanian P. Role of vitamin D in the outcome of ischemic stroke- a randomized controlled trial. J Clin Diagn Res. 2017;11(2):CC06-CC10.
doi pubmed - Afshari L, Amani R, Soltani F, Haghighizadeh MH, Afsharmanesh MR. The relation between serum Vitamin D levels and body antioxidant status in ischemic stroke patients: A case-control study. Adv Biomed Res. 2015;4:213.
doi pubmed - Aggarwal HK, Jain D, Pahuja T, Singh J, Dahiya S. Vitamin D as a predictor of severity and prognosis of acute ischemic stroke. Turkish Journal of Neurology. 2022;28(3):142-147.
- Alfieri DF, Lehmann MF, Oliveira SR, Flauzino T, Delongui F, de Araujo MC, Dichi I, et al. Vitamin D deficiency is associated with acute ischemic stroke, C-reactive protein, and short-term outcome. Metab Brain Dis. 2017;32(2):493-502.
doi pubmed - Borowicz W, Ptaszkowski K, Ptaszkowska L, Rosinczuk J, Murawska-Cialowicz E. Association between serum vitamin D levels and physical outcomes of patients who underwent rehabilitation following ischemic stroke. Med Sci Monit. 2023;29:e940115.
doi pubmed - Rad RE, Zarbakhsh M, Sarabi S. The relationship of vitamin D deficiency with severity and outcome of acute stroke. Rom J Intern Med. 2021;59(4):351-358.
doi pubmed - Samarakoon N, Chang T, Gunasekara V, Ratnayake P, Jayatillake R, Udagama P. Selected serum cytokines and vitamin D levels as potential prognostic markers of acute ischemic stroke. PLoS One. 2024;19(6):e0299631.
doi pubmed - Turetsky A, Goddeau RP, Jr., Henninger N. Low serum vitamin D is independently associated with larger lesion volumes after ischemic stroke. J Stroke Cerebrovasc Dis. 2015;24(7):1555-1563.
doi pubmed - Wajda J, Swiat M, Owczarek AJ, Brzozowska A, Olszanecka-Glinianowicz M, Chudek J. Severity of vitamin D deficiency predicts mortality in ischemic stroke patients. Dis Markers. 2019;2019:3652894.
doi pubmed - Kim C, Lee SH, Lim JS, Kim Y, Jang MU, Oh MS, Jung S, et al. Impact of 25-hydroxyvitamin D on the prognosis of acute ischemic stroke: machine learning approach. Front Neurol. 2020;11:37.
doi pubmed - Park KY, Chung PW, Kim YB, Moon HS, Suh BC, Won YS, Kim JM, et al. Serum vitamin D status as a predictor of prognosis in patients with acute ischemic stroke. Cerebrovasc Dis. 2015;40(1-2):73-80.
doi pubmed - Alharbi AR, Alali AS, Samman Y, Alghamdi NA, Albaradie O, Almaghrabi M, Makkawi S, et al. Vitamin D serum level predicts stroke clinical severity, functional independence, and disability-A retrospective cohort study. Front Neurosci. 2022;16:951283.
doi pubmed - Acharya SS, Mishra S, Padhy RK, Malini DS. A randomized control trial on effect of vitamin D in stroke in a tertiary care hospital of Southern Odisha. European Journal of Molecular & Clinical Medicine. 2022;9(7):838-848.
- Zielinska-Nowak E, Cichon N, Saluk-Bijak J, Bijak M, Miller E. Nutritional supplements and neuroprotective diets and their potential clinical significance in post-stroke rehabilitation. Nutrients. 2021;13(8):2704.
doi pubmed - Atif F, Yousuf S, Espinosa-Garcia C, Harris WAC, Stein DG. Post-ischemic stroke systemic inflammation: Immunomodulation by progesterone and vitamin D hormone. Neuropharmacology. 2020;181:108327.
doi pubmed - Yousuf S, Atif F, Espinosa-Garcia C, Harris W, Turan N, Stein DG. Stroke-induced peripheral immune dysfunction in vitamin D-Deficient conditions: modulation by progesterone and vitamin D. Mol Neurobiol. 2021;58(3):950-963.
doi pubmed - Hesami O, Iranshahi S, Shahamati SZ, Sistanizd M, Pourheidar E, Hassanpour R. The evaluation of the neuroprotective effect of a single high-dose Vitamin D(3) in patients with moderate ischemic stroke. Stroke Res Treat. 2022;2022:8955660.
doi pubmed - Safari A, Fadakar N, Borhani-Haghighi A. The association between inflammatory biomarkers and vitamin D level with the evolution and severity of stroke. Basic Clin Neurosci. 2022;13(6):807-814.
doi pubmed - Pinzon RT, Christina NS, Sugianto OY, Primastuti TF. Correlation between vitamin D levels and cognitive impairment on 90 days post ischemic stroke patients. Romanian Journal of Neurology. 2022;21(3):237.
- Morris-Blanco KC, Chokkalla AK, Kim T, Bhatula S, Bertogliat MJ, Gaillard AB, Vemuganti R. High-dose vitamin C prevents secondary brain damage after stroke via epigenetic reprogramming of neuroprotective genes. Transl Stroke Res. 2022;13(6):1017-1036.
doi pubmed - Rist PM, Buring JE, Cook NR, Manson JE, Rexrode KM. Effect of vitamin D and/or omega-3 fatty acid supplementation on stroke outcomes: A randomized trial. Eur J Neurol. 2021;28(3):809-815.
doi pubmed - Rezaei O, Ramezani M, Roozbeh M, Fazeli B, Hajiesmaeili M, Pakdaman H, Simani L. Does vitamin D administration play a role in outcome of patients with acute ischemic stroke? A randomized controlled trial. Curr J Neurol. 2021;20(1):8-14.
doi pubmed - Kadri A, Sjahrir H, Juwita Sembiring R, Ichwan M. Combination of vitamin A and D supplementation for ischemic stroke: effects on interleukin-1ss and clinical outcome. Med Glas (Zenica). 2020;17(2):425-432.
doi pubmed - Selim FO, Fahmi RM, Ali AE, Raafat N, Elsaid AF. Serum vitamin D levels in acute stroke patients. The Egyptian Journal of Neurology, Psychiatry and Neurosurgery. 2019;55:1-8.
- Torrisi M, Bonanno L, Formica C, Arcadi FA, Cardile D, Cimino V, Bramanti P, et al. The role of rehabilitation and vitamin D supplementation on motor and psychological outcomes in poststroke patients. Medicine (Baltimore). 2021;100(45):e27747.
doi pubmed - Sari A, Durmus B, Karaman CA, Ogut E, Aktas I. A randomized, double-blind study to assess if vitamin D treatment affects the outcomes of rehabilitation and balance in hemiplegic patients. J Phys Ther Sci. 2018;30(6):874-878.
doi pubmed - Simon J, Sriharsha T, Perumal Kumaresan A, Chand U, Bose S. Impact of vitamin D deficiency on ischemic stroke severity: insights from a prospective study. Cureus. 2024;16(9):e69376.
doi pubmed - Daubail B, Jacquin A, Guilland JC, Hervieu M, Osseby GV, Rouaud O, Giroud M, et al. Serum 25-hydroxyvitamin D predicts severity and prognosis in stroke patients. Eur J Neurol. 2013;20(1):57-61.
doi pubmed - Fahmy E, Sharaf S, Helmy H, Sherif S. Vitamin D status in acute ischemic stroke: relation to initial severity and short-term outcome. The Egyptian Journal of Neurology, Psychiatry and Neurosurgery. 2019;55:1-6.
- Tu WJ, Zhao SJ, Xu DJ, Chen H. Serum 25-hydroxyvitamin D predicts the short-term outcomes of Chinese patients with acute ischaemic stroke. Clin Sci (Lond). 2014;126(5):339-346.
doi pubmed - Wang Y, Ji H, Tong Y, Zhang ZB. Prognostic value of serum 25-hydroxyvitamin D in patients with stroke. Neurochem Res. 2014;39(7):1332-1337.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Neurology Research is published by Elmer Press Inc.